
Volume 18, Issue 1 (5-2021)
J Res Dev Nurs Midw 2021, 18(1): 9-12 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mancheri H, Sabzi Z, Alavi M, Vakili M A, Maghsoudi J. The Quality of Life of Women with Addicted Husbands and its Related Factors in Gorgan, Iran. J Res Dev Nurs Midw 2021; 18 (1) :9-12
URL: http://nmj.goums.ac.ir/article-1-1121-en.html
URL: http://nmj.goums.ac.ir/article-1-1121-en.html



1- Student Research Committee, School of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran
2- Faculty of Nursing & Midwifery, Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran
3- Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran
4- Development Research Center, Department of Biostatistics and Epidemiology, Faculty of Health, Golestan University of Medical Sciences, Gorgan, Iran
5- Psychiatric and Mental health Nursing Department, Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran , maghsoudi@nm.mui.ac.ir
2- Faculty of Nursing & Midwifery, Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran
3- Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran
4- Development Research Center, Department of Biostatistics and Epidemiology, Faculty of Health, Golestan University of Medical Sciences, Gorgan, Iran
5- Psychiatric and Mental health Nursing Department, Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran , maghsoudi@nm.mui.ac.ir
Keywords: Quality of Life [MeSH], Behavior [MeSH], Addictive [MeSH], Substance-Related Disorders [MeSH], Spouses [MeSH], Women [MeSH]
Full-Text [PDF 659 kb]
(1190 Downloads)
| Abstract (HTML) (2518 Views)
Abstract
Full-Text: (633 Views)
Abstract
Background: Substance abuse can cause problems for family members, especially spouses, and impair the addicts' quality of life; hence, it seems necessary to identify issues that can endanger their quality of life and health. Therefore, the present study aimed to determine the quality of life of women with addicted husbands, and its related factors.
Methods: We conducted the present cross-sectional study on 300 women with addicted husbands who were in the list of clients of private and public addiction treatment centers in Gorgan in 2018. The convenient sampling was used for recruited participants. We gathered data using the World Health Organization Quality of Life-BREF (WHOQOL-BREF), the higher scores indicated a better quality of life. We also analyzed the data in SPSS 16 using descriptive statistics, Chi-square and Mann-Whitney tests at a 95% confidence interval.
Results: The results indicated that women with addicted husbands had lower mean scores of physical health (33.3±19.1), mental health (28±3.19), environmental health (31.5±18.1), social relationship (30.2±21.4), and total scores of quality of life (31±18). There were significant correlation between scores of quality of life and its dimensions with women's job, family income, duration of substance abuse, and type of substance (P<0.001). Also, the quality of life was directly associated with women's jobs and family income, but inversely related to the husband's duration of substance abuse and type of substance.
Conclusion: Women with addicted husbands needed more support due to their low quality of life. These findings help the healthcare provider pay more attention to the problems of women with addicted husbands.
Introduction
Substance dependence is an important social issue in the world. The World Health Organization (WHO) estimates that there are approximately two hundred and thirty million addicts worldwide, accounting for about 5% of the world's population (1). According to studies, almost 37% of the US population over the age of 12 have experienced the substance abuse at least once. According to the report, the highest prevalence of substance abuse (2.8%) was among the Iranians aged 15 to 64 (2).
The substance dependence generally causes serious harm to individuals, families, and society, and also incurs heavy costs for families and countries (3). In the family system, the substance abuse has negative effects, especially on the spouse, parents, and children of substance abuser (4) so that it reduces the quality of life of family members (5). Quality of life is a health variable that provides high levels in life, peace, and happiness. The WHO defines the quality of life as the individuals' perceptions of their situations in terms of cultural conditions and values in which they live. The more positive and better these perceptions are, the higher the quality of life a person has, and vice versa. Researchers have considered two main characteristics for quality of life, namely the happiness and satisfaction. In other words, the individuals' perception of levels of happiness and satisfaction in dimensions of life determines the levels of quality of life (6).
Health is considered as an important domain in most definitions of quality of life, but when people are asked to define important domains of the quality of life, it is considered as a primary domain. A qualitative study on the concept of quality of life indicated that social belonging and self-care were as composite factors of quality of life. Furthermore, some quantitative studies have identified health-related issues as determinants of quality of life, indicating the probability of impact of health status on the concept of quality of life (7).
Undoubtedly, addiction is a factor that undermines the basis of individual life and causes family disputes. The harmfulness of the current situation increases when the spouses of addicted people become aware of their spouses' conditions. In such situations, their spouses lose their life expectancy, their mental well-being, and social relationships and quality of life are disrupted. In summary, sadness, grief, loneliness, shame, and psychological insecurity dominate their lives (8). Gehlawat et al. (2014) found that the substance abuse caused severe confusion in family members and those who cared for them, especially their spouses (9). Najafi et al. (2005) also found that the quality of life of women, who had addicted husbands, was low (10). Women in families with addicted husbands might face the most pressures from all sides and alone bear the overall responsibility of a troubled family (11). In addition to housework and raising children, the woman in the family has to take the responsibility of finances and care of the family. They are also exposed to a variety of harms from substance abuse. Bitter evidence of emotional breakdown, divorce, and disintegration of the family hearth are among the adverse effects of this category. Looking at the structure of problematic families, including addicted families occur with the lack of proper communication between couples, turmoil and conflicts between family members. Addicted spouses show mostly negative and vulnerable relationships such as criticism, blame, humiliation, and anger, and express a low level of empathy in resolving family problems. Negative relationships reduce the use of problem-solving skills, and the family declines functionally; hence, the declining family performance leads to the fall and destruction of the family health (12).
The presence of a drug addict in the family affects various aspects of the family; the family members of the addicted person seriously feel defeated and experience negative emotions. Furthermore, families try to adapt to the problems that arise by using strategies of denial and aggression (13). Therefore, living with a person, who is substance abuser or drinks alcohol, is stressful. A person, who has a substance abuse problem, often takes actions that can adversely affect the family life and family members of addicted person (14), and it ultimately increases the burden of health care in these families. The results indicate that the use of health care services by these families is four times higher than the normal families (15).
Given that addiction is an ominous social phenomena, it not only has adverse effects on the life of addicts, but also puts their relatives and friends at risk of various harms of this social phenomenon. There are few studies on the quality of life of women with addicted husbands, but much studies have been done on addiction and their families, and all of them have been on the psychological, social, and communicational problems of the families. Due to the importance of the concept of quality of life, and its role in the individuals' social and mental health, and the fact that the substance abuse can cause problems for family members, especially their spouses, and cause disruption in the process of their quality of life, it is significantly important to investigate the quality of life spouses of addicts because if their quality of life is ignored, they will have hopelessness, lack of motivation, and lower social, economic, cultural, and health activities that deeply affect the social progress. Furthermore, the study of spouses' quality of life can also be considered from two other aspects: first, effects of harms can be prevented by recognizing them; secondly, this group can support the patients in the process of intoxication and encourage them to continue this way (10). In fact, examining the individuals' quality of life and taking efforts to improve and enhance it will increase the individuals' physical and mental health. Accordingly, we conducted a study with an aim to determine the quality of life of women with addicted husbands and its related factors.
Methods
We conducted the present cross-sectional study on women with addicted husbands in 2018 for five months (from May to September). Samples were selected from women whose husbands visited public and private addiction treatment centers in Gorgan by a convenience sampling method. In Gorgan, there are a public center and 70 private addiction treatment centers. After obtaining official permission from the ethics committee of the university and also the deputy of treatment of Golestan University of Medical Sciences, we visited the addiction treatment centers (a public center and 20 private centers). We selected 300 samples using the convenience sampling method after preparing a list of clients in the addiction treatment centers. We prepared the list of clients only to identify the eligible individuals for the research, and any sample with the inclusion criteria was included in the research. Inclusion criteria: no substance abuse and known physical and psychiatric disorders in the samples. We utilized the demographic information registration form, including the participants' age, education levels, and job, family income, residential status, variety of husband's drug, and its duration) and the World Health Organization Quality of Life-BREF (WHOQOL-BREF) to collect the data. The questionnaire, which was developed by a group of experts from the World Health Organization in 1996 by modifying the items of a 100-question form of the questionnaire, measures the overall quality of life. This questionnaire has 4 subscales, physical health, mental health, social relationships, and environmental health (16).
The physical health domain (8 items, including questions 3, 4, 10, 15, 16, 17, and 18), mental health (6 items, including questions 5, 6, 7, 11, 19, and 26), environmental health (7 items, including questions 8, 9, 12, 13, 14, 23, 24, and 25), and social relations (3 items, including questions 20, 21, and 22) ask 24 questions. The first two questions do not belong to any of the domains, and they generally assess the health and quality of life. Therefore, the questionnaire has a total of 26 questions. The questionnaire items are also evaluated on a 5-item scale each which receives a score of 1 to 5. Initially, a raw score is obtained for each subscale and becomes a standard score between 0 and 100. A score of 0-30 indicates an unfavorable quality of life, a score of 30-70 indicates a medium quality of life, and a score of 70-100 indicates a better and more desirable quality of life (17). A score of 0 to 100 was considered for each domain to compare the scores of the domains with each other according to the following equation (18).
Yi = Xi−minXXX /max (Xi) −XXX
Validity and reliability of the tool were performed by Nejat et al. in a study, titled "Standardization of the World Health Organization Quality of Life-BREF (WHOQOL-BREF): Translation and psychometrics of the Iranian species; and the questionnaire had good validity. The Cronbach's alpha values between the four domains were 0.73 for obtaining the reliability (19).
After obtaining the necessary permission from Golestan University of Medical Sciences and obtaining an official permission from the Ethics Committee of the University to attend Gorgan Addiction Treatment Centers, the researcher visited the centers and introduced himself to research units after selecting them, and then he explained the research purpose. After obtaining the written consent from the samples, the questionnaires and information registration forms were completed in the presence of the researcher and through interviews.
The data were provided in SPSS statistics for windows, version 16.0 (SPSS Inc., Chicago, III., USA) using descriptive statistics, including mean, standard deviation, frequency, and percentage. To analyze the data, first the normality conditions were examined for the quantitative variables, and the independent t-test was used if the conditions were met, otherwise the Mann-Whitney test was used. Chi-square test was also used for classified variables. Pearson correlation test examined the correlation between domains of quality of life.
Results
The results indicated that the highest age frequency of women participating in the study belonged to the age range of over 40 years (29%), most of whom (54%) had under high school diploma, were housewives (51%), had low income (75.3%), and lived in rented houses (47.6%). In terms of variety of husbands' drugs, 142 husbands (47.4%) had a history of consuming two types of substances (Table 1). Due to the lack of normality of total quality of life scores in different subgroups of independent variables, the Kruskal-Wallis nonparametric test indicated no statistical significant relationship between total scores of quality and age of women (P=0.295), educational status of women (P=0.251), and family housing status (P=0.293) (P>0.05), while there was a significant relationship between the husbands' duration of substance abuse and the total score of quality of life (P=0.038). There was also a significant relationship between women's jobs and total quality of life score (P<0.001) (Table 1). The difference belonged to the job groups of daily wage with housewife and also daily wage with employee. Women, who had to work to earn a living, had a worse quality of life. Mann-Whitney nonparametric test also indicated that there was a significant relationship between family income and total quality of life score (P<0.001) so that a family with lower income had worse living conditions. Kruskal-Wallis test also indicated that there was a significant relationship between the variety of substances and the total score of quality of life (P<0.001). Women whose husbands had a history of abusing more than one type of substance, had a lower quality of life.
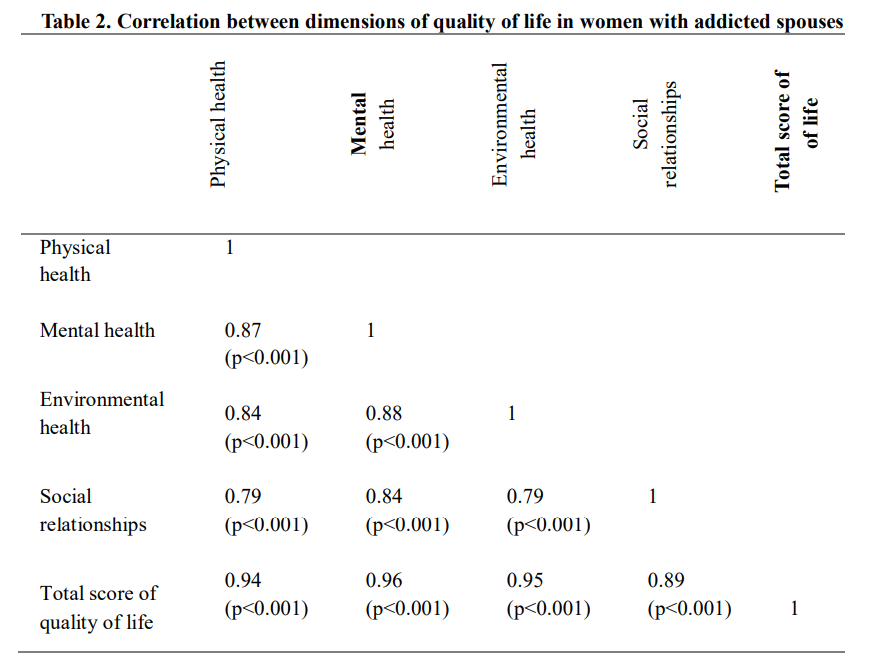
The results also indicated that the mean scores of physical health (33.3±19.1), mental health (28±3.19), environmental health (31.5±18.1), social relations (30.2±21.4) as well as the total score of quality of life (31±18) of women with addicted husbands were low in the study, and the lowest score belonged to mental health, and the highest score belonged to physical health. There was a direct and positive correlation between dimensions of quality of life (physical health, mental health, environmental health, and social relationships) with together, and with the total score of quality of life. The mental health dimension had the highest correlation, and the social relationships dimension had the lowest correlation with the total score of quality of life (Table 2).

Discussion
According to the research results, the quality of life of women with addicted husbands was at a low level. The results were consistent with findings of many studies, indicating that addiction decreased the quality of life, and increased psychological and social problems for them. Navabi et al. (2017) extracted experiences about the quality of life from addicted families and classified them into seven main topics, including financial issues, intercourse disability, physical, emotional, social, and mental health, and performance-related issues. The quality of life of family members of addicts was low and it was consistent with the present study (20).
In Najafi's study, the mean score of the GHQ28 was 28.5 in the group of women with addicted husbands and, and 13.3 in the control group; and the women had lower general health than the control group (P= 0.002, and T= 3.3). The women with addicted husbands had lower levels of general health in terms of symptoms of depression, somatic disorders, anxiety, insomnia, and social performance in comparison with the control group, and the difference was significant in depression, anxiety, and insomnia and somatic disorders (P <0.001).
The present study indicated that women with addicted husbands had low levels of mental health, and the result was consistent with studies by Mahdizadeh (21). Mariarty et al. (2011) (22), Mancheri et al. (2013) (23), and Keshavarz et al. (2014) (24). Addiction is a family illness, and after years of enduring the anxiety of living with an addicted person, family members, especially the addicted person's spouse, may be in a much worse psychological state than the addicted person. The sad truth is that the addicted person drowns in the drunkenness caused by the substance abuse, and does not know what problems the addiction will bring for oneself or family. The addict's family members have no choice but to endure the problems that the addicted person has created for them, and since they have no available support to bring comfort and peace of mind, they further feel the devastating and terrifying effects of the family member's addiction. Even if the addict stops using the drug and is recovering, family members will still be affected by the psychological and emotional damage left from the addiction time. As long as the family members do not accept that their own lives are affected by the addiction and need a solution to recover, they will undoubtedly continue the same painful and unhealthy life that they have been accustomed to for many years with an addicted person (25).
In the present study, the mean score of spouses in physical dimension was 33.3 that was a low level. Choudhary (2016) (26), Ray et al. (2008) (27), and lee et al. (2011) (15) found that family members of addicts had physical problems probably since living with substance abusers was stressful. Substance abusers often take actions that can adversely affect their own and family members' lives (14).
Addiction is an ominous social phenomena and the importance of the women's role in families with addicted heads doubles since that the family is the most vulnerable social institution to effects of addiction and the addicted head is not able to play his role as a husband or father due to addiction. Given that this group of women are among the most vulnerable groups in society, they are exposed to serious physical, psychological, social, and economic harm (21).
Family therapy theories indicate that the family is a whole and the whole family system should be taken into consideration to solve the problem of family or a member because the performance of the family and the individual are interdependent and individual problems reflect the family problems and vice versa (28). Addiction is no exception to this rule, the harms of addiction are transmitted to the family in addition to the consumer; hence, women with addicted husbands are, on the one hand, facing with cultural and social challenges, and on the other hand, with economic and livelihood problems. These problems reduce the quality of life, frustration for the uncertain future of themselves and their children (29).
Most spouses had low scores of social relationships, and the result was consistent with studies by Mancheri et al. (2013) (23), Lander Et al. (2013) (30), and Daley (2013) (31). Being in a tight spot for social relationship is a theme that Nikbakht raised in his study on the experiences of women with addicted husbands. According to most participants, this problem occurs in wives due to the negative attitude of society towards addiction. Exposure to unpleasant and sometimes immoral behaviors and speeches of the society, such as labeling it "practical", people's distrust due to the social stigma of addiction, led to the theme. Most of the participants mentioned that the stigma of their husbands' addiction led to their lower self-confidence, feeling of inadequacy, and social isolation, indicating the heavy burden of the social stigma of addiction in society as the stigma of addiction caused the wife to be forced to leave the social situations of the family and deprive herself of society and the pleasure of social communication (11).
In the present study, it was also found that there was a positive and significant correlation between dimensions of quality of life (p<0.001), and it was consistent with a study by Vaez (2004) (32) and Soltani (2010) (33). The mental health dimension had the highest correlation and the social relationship dimension had the lowest correlation with the total score of quality of life. Falahzade et al. (34) found that the mental health had the highest correlation with quality of life, but they found that the environmental health dimension had the least correlation with quality of life. It can be concluded that poor quality of life in one domain leads to lower quality in other domains of quality of life, and thus all four dimensions of quality of life should be taken into consideration to increase the quality of life of women with addicted husbands.
In the present study, there was a significant relationship between quality of life score and its dimensions with some demographic characteristics such as women's job, family income, duration of substance abuse, and whether the consumer used one type or several types of substance (p <0.001), but they had no significant relationship with women's age, educational level, and housing status. In the field of the quality of life score with their job status and the lack of relationship with their educational levels and age, the findings were consistent with a study by Mancheri et al. (2013) who found that working women had a better psychological and social status than women who were not employed (13). For the relationship of quality of life score with type of substance, the finding as consistent with a study by Narimani et al. (2014) who found that the quality of life of the children of heavy drug abusers was lower than the quality of life of the children of light substance abusers. According to the finding, heavy substance abuse by parents had a more destructive effect on the family structure, including the high rate of divorce among the families (5), but in a study by Najafi et al., the demographic characteristics, including family income, job, and housing status, were similar between the two groups and there was no statistically significant difference (10).
In their study, there was no statistically significant difference between demographic characteristics, including family income, and job with quality of life between the two groups (women with addicted husbands, and women without addicted husbands) (10), and the result was inconsistent with findings of the present research probably due to personal, cultural, and research society differences.
Conclusion
Low quality of life in families, especially women with addicted husbands, need comprehensive understanding and support. The findings give a new perspective to the treatment team to have a more realistic understanding of the families of addicts and their real problems. Given the low quality of life in all dimensions, it is a basic necessity to develop educational and intervention programs to improve the quality of life of women with addicted husbands.
Acknowledgements
The present article was derived from a doctoral dissertation at Isfahan University of Medical Sciences and a joint research project with the Nursing Research Center of Golestan University of Medical Sciences with the code of ethics (IR.GOUMS.REC.1397.211). The researchers are grateful to women with addicted husbands, personnel of the addiction treatment centers, and officials who helped us in the study.
Funding source
This research did not receive any grant from funding agencies.
Ethical statement
This study was approved by the ethics committee of the Golestan University of Medical Sciences.
Conflict of interest
The authors declared no conflict of interest.
Author contributions
Conceptualization: Hamideh Mancheri, Jahangir Maghsoudi. Methodology, analysis, research review and editing: Hamideh Mancheri, Jahangir Maghsoudi, Zahra Sabzi, Mousa Alavi and Mohammad Ali Vakili.. Writing: Hamideh Mancheri. Supervision: Jahangir Maghsoudi.
Type of Study: Original Article |
Subject:
Management and Health System
References
1. Yousefi Afrashteh M, Amiri M,Morovati Z, Babamiri M, CHeraghi A. Supporting factors of constancy in quitting drugs: A qualitative study. J Qual Res Health Sci . 2015; 4(3):280-9. [View at paplisher] [Google Scholar]
2. Afkar A, Rezvani S, Emami Sigaroudi A. Measurement of Factors Influencing the Relapse of Addiction: A Factor Analysis. J High Risk Behav Addict. 2017; 6(3):1-8. [View at paplisher] [DOI] [Google Scholar]
3. Senthil M, Kiran M. Relationship between Family Interaction pattern, Family Burden and Quality of Life among Caregivers of Patients with Alcohol Dependence. The International Journal of Indian Psychology. 2016; 3(4):107-13. [View at paplisher] [DOI]
4. Copello AG, Velleman RD, Templeton LJ. Family interventions in the treatment of alcohol and drug problems. Drug Alcohol Rev. 2005; 24(4):369-85. [View at paplisher] [DOI] [Google Scholar]
5. Narimani M, Alaei S, Hajloo N, Abolghasemi A. Study of Different Dimensions of Quality of Life in the Children of Addicted People. Rural development. 2014; 6(1):1-17. [View at paplisher] [Google Scholar]
6. Robert J. Sternberg and and James C. Kaufman. Human abilities. Annual Review of Psychology.1998; 49:479- 502. [View at paplisher] [DOI:10.1146/annurev.psych.49.1.479]
7. Maeyer JD, Vanderplasschen W, Lammertyn J, Nieuwenhuizen CV, Sabbe B, Broekaert E. Current quality of life and its determinants among opiate-dependent individuals five years after starting methadone treatment. Qual Life Res. 2011; 20:139-50. [View at paplisher] [DOI:10.1007/s11136-010-9732-3] [Google Scholar]
8. Tarkhan M. The effectiveness of short-term group interpersonal therapy on the psychological well-being and the life quality of addicted individuals' wives. Quarterly Journal of Educational Psychology. 2011; 2(1):23-36. [View at paplisher] [Google Scholar]
9. Gehlawat P, Singh P, Gehlawat VK. Family Burden in Substance Use Disorders. International Journal of Scientific Research. 2014; 3(3):292-4. [View at paplisher] [DOI:10.15373/22778179/MARCH2014/98]
10. Najafi K, Zarrabi H, Kafi M, Nazifi F. Compare the Quality of Life of Spouses of Addicted Men with a Control Group. Guilan University of Medical Sciences. 2005; 14(55):35-41. [persian] [View at paplisher] [Google Scholar]
11. Nikbakht Nasrabadi AR, Pashaei sabet F, Bastami AR. Life experiences of addicted wife:A qualitative study. Iranian journal of nursing research. 2016; 11(1):62-75.[persian] [View at paplisher] [Google Scholar]
12. Mohammadifar M, Talebi A, Tabatabai SM. Effect of life skills training on family function in women with addicted spouse. Drug addiction study checklist. 2011; 4(16):25-39. [View at paplisher] [Google Scholar]
13. Mancheri H, Sharifi Neyestanak N, Seyedfatemi N, Heydari M, Ghodoosi M. Psychosocial Problems of Families Living with an Addicted Family Member. IJN. 2013; 26 (83):48-56. [PERSIAN] [View at paplisher] [Google Scholar]
14. Velleman R, Templeton L. Alcohol, drugs and the family: results from a long-running research programme within the UK. European Addiction Research. 2003; 9(3):103-12. [View at paplisher] [DOI:10.1159/000070978] [Google Scholar]
15. Lee KMT, Manning V, Teoh H, Winslow M, Lee A, Subramaniam M, et al. Stress‐coping morbidity among family members of addiction patients in Singapore. Drug Alcohol Rev. 2011; 30(4):441-7. [View at paplisher] [DOI:10.1111/j.1465-3362.2011.00301.x] [Google Scholar]
16. Taghinegad H, Azadi A, Jamaledin H, Azizi M. The Role of stressors in the prediction of procrastination and academic burnout among the Nursing Students of Ilam University of Medical Sciences in 2015. Scientific Journal of Nursing, Midwifery and Paramedical Faculty. 2016; 2(2):1-8. [Persian] [View at paplisher] [DOI:10.29252/sjnmp.2.2.1] [Google Scholar]
17. Azizi M, Baroony zadeh Z, Motamedzade M, Goli S. Study of Nurses Quality of Life using WHO Questionnaire in Hospitals of Hamadan University of Medical Sciences. Journal of Occupational Hygiene Engineering. 2015; 1(4):68-75. [Persian]
18. Derakhshanpour F, Vakili M, Farsinia M, Mirkarimi K. Depression and Quality of Life in Patients with Type 2 Diabetes. Iran Red Crescent Med J. 2015; 17(5):1-6. [View at paplisher] [DOI:10.5812/ircmj.17(5)2015.27676] [Google Scholar]
19. Nejat S, Montazeri A, Holakouie Naieni K, Mohammad K, Majdzadeh S. The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version. Journal of the School of Public Health and Institute of Public Health Research. 2006; 4 (4):1-12 [View at paplisher] [Google Scholar]
20. Navabi N, Asadi A, Nakhaee N. Impact of Drug Abuse on Family Quality of Life. Addict Health. 2017; 9(2):118-9. [View at paplisher] [Google Scholar]
21. Mahdizadeh S, Ghoddoosi A, Naji S. Investigation of Internal Tensions of Wives of Men Who Addicted to Heroin. AUMJ. 2013; 2(3):128-38.[Persian] [View at paplisher] [DOI] [Google Scholar]
22. Moriarty H, Stubbe M, Bradford S, Tapper S, Lim B. Exploring resilience in families living with addiction. J of primary health care. 2011; 3(3):210-7. [View at paplisher] [DOI] [Google Scholar]
23. Mancheri H, heidari M, Ghodusi Borujeni M. Correlation of Psychosocial problems with perception of social support families with addicted member admitted. IJPN. 2013; 1 (3):1-9. [View at paplisher] [Google Scholar]
24. Keshavarz M, ghomrani A, Bagherian M, Rezae AM. Examination of the religious orientation and burden of family as predictors of treatment permanence of addiction. RBS. 2014; 12(1):144-53. [Persian] [View at paplisher] [Google Scholar]
25. Mortelmans D, Snoeckx L, Dronkers J. Cross-Regional Divorce Risks in Belgium: Culture or Legislative System. Journal of Divorce & Remarriage. 2009; 50(8):541-63. [View at paplisher] [DOI] [Google Scholar]
26. Choudhary M. A Qualitative Study to assess Perceived Burden among Caregivers of Client with Substance Dependence. IJNER. 2016; 4(2):169-73. [View at paplisher] [DOI] [Google Scholar]
27. Ray GT, Mertens JR, Weisner C. Family members of people with alcohol or drug dependence: health problems and medical cost compared to family members of people with diabetes and asthma. Addiction. 2008; 104(2):203-14. [View at paplisher] [DOI] [Google Scholar]
28. Minochin S. Family and Family Therapy, Translated by Bagher Sanaie Zaker. Tehran: Amir Kabir. 2013. 351P.
29. Naemi AM. Effectiveness of family-based education on mental health and resiliency of women with addicted husband (Case study: Sabzevar). Wom Dev Pol. 2015; 1(13):4-52. [View at paplisher] [Google Scholar]
30. Lander L, Howsare J, Byrne M. The impact of substance use disorders on families and children: from theory to practice. Soc Work Public Health. 2013; 28(3-4):194-205. [View at paplisher] [DOI] [Google Scholar]
31. Daley D. Family and social aspects of substance use disorders and treatment. J Food Drug Anal. 2013; 21(4):S73-S6. [View at paplisher] [DOI] [Google Scholar]
32. Vaez M, Kristenson M, Laflamme L. Perceived Qoulity of Life and Self-rated Health Among First-Year University Students.Social Indicators Research. 2004; 68(2):221_34. [View at paplisher] [DOI] [Google Scholar]
33. Soltani R, Kafee SM, Salihi I, Karashki H, Rezaee S. Survey the Quality of Life in Guilan University Students. Jour Guilan Uni Med Sci. 2010; 19(75):25-35. [Persian] [View at paplisher] [Google Scholar]
34. Falahzade H, Shokohifar M, Askarishahi M, Morowati Sharifabad M, Afkhami Ardakani M. Evaluating Life Quality in Type II Diabetic Patients Compared to Healthy People and Presentating a Structural Model. TB. 2015; 14 (4):78-87. [Persian] [View at paplisher] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
