
Volume 16, Issue 1 (1-2019)
J Res Dev Nurs Midw 2019, 16(1): 33-42 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirhadyan L, Molaee S, Mosaffay Khomami H, Kazem Nejad Leili E. Health Promoting-behaviors and its Relation with the Risk of Type 2 Diabetes in Women Referred to Community Health Centers in Rasht. J Res Dev Nurs Midw 2019; 16 (1) :33-42
URL: http://nmj.goums.ac.ir/article-1-1100-en.html
URL: http://nmj.goums.ac.ir/article-1-1100-en.html



1- instructor, Shahid Beheshti Nursing and Midwifery Shool of Rasht, social determinates of health research center
2- student, Shahid Beheshti Nursing and Midwifery Shool of Rasht, social determinates of health research center.
3- Associate professor, Shahid Beheshti Nursing and Midwifery Shool of Rasht, social determinates of health research center.
2- student, Shahid Beheshti Nursing and Midwifery Shool of Rasht, social determinates of health research center.
3- Associate professor, Shahid Beheshti Nursing and Midwifery Shool of Rasht, social determinates of health research center.
Full-Text [PDF 795 kb]
(2211 Downloads)
| Abstract (HTML) (9696 Views)
Table 2- The mean and standard deviation of the dimensions of health promotion behaviors in the groups at risk for type 2 diabetes in the studied samples
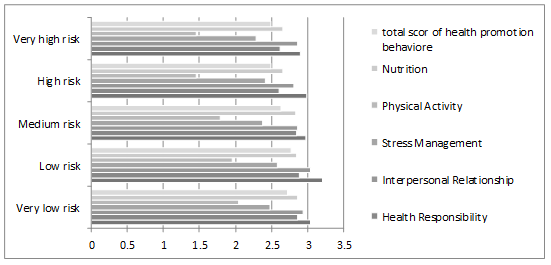
Diagram 1: Average Score of Health Promotion Behavioral Dimensions In groups at risk for type 2 diabetese
Discussion
The women of this study showed a moderate level of health-promoting behaviors. In a large number of studies that examined the health-promoting behaviors in the women's population, similar results were obtained (17), (18), (19), and (20). Women's health should be an important aspect of advancement in societies and health policies, and policymakers and health providers should plan and intervene to promote health in this target group. The total mean score of health-promoting behaviors in the five groups at risk for type 2 diabetes was different so that the lowest and highest risk groups received the lowest score. Compared to the five groups, this difference was statistically significant, which indicates that the status of the health-promoting behaviors in the low-risk group is desirable but in the high-risk group of type II diabetes is undesirable. In Chen's study, people at risk for metabolic syndrome had better health-promoting behaviors than those with metabolic syndrome (21). In addition, in the Wu’s study, in general, the samples showed a moderate level of health-promoting behaviors, and the healthy participants had higher levels of health-promoting behaviors than those with metabolic syndrome (22). El mokadem in his study found that there was a statistically significant difference between the score of health-promoting behaviors and the risk score for cardiovascular disease (diabetes and hypertension) in women (23). However, Sutherland who examined the health-promoting behaviors with regard to the risk of diabetes found that the average score of health-promoting behaviors in the natural group was lower than the diabetic group (12). Furthermore, in Sorour's study, there was no significant relationship between the mean score of health-promoting behaviors and chronic illnesses (24). Differences in results may be related to the type of research and tools used and the difference in the research samples.
The results indicate that there is a relationship between women's health-promoting behaviors and their risk of developing type 2 diabetes over the next ten years (26). More attention of policy makers and health service providers is essential for promoting women's health as one of the major dimensions of community development. Findings of the research regarding the dimensions of health-promoting behaviors indicate that the highest mean score in self-actualization dimension is in line with many similar studies (18), (12), and (26). Self-actualization, which is a psychological factor influencing the realization of the potential ability of individuals to "get the best", is a health-promoting factor (17). The Iranian women's religion is an influential factor in self-actualization. In the review of different studies, there was a difference in dimensions that had the highest average score due to differences in cultures and factors influencing health-promotion behaviors and the different units of the research. However, in most studies, the highest mean score is related to self-actualization and interpersonal relationships influenced by culture and religion. In most studies, the lowest mean score was related to exercise. The result was consistent with the results of some studies (27), (12), (26), (21) which could be related to the industrial lifestyle. This kind of lifestyle has become a problem for many countries because the positive impact of physical activity on health is undeniable. Physical inactivity is a major risk factor for pre-diabetes. Physical activity is essential for women and physical inactivity makes them susceptible to cardiovascular disease and diabetes (28).
Based on the findings, except for the mean score of interpersonal support, the scores of other dimensions in terms of the risk groups of type 2 diabetes were statistically significant. The score of health-promoting behaviors in all studied areas has a descending trend from low-risk and very low-risk groups to high-risk and very high-risk groups. These findings suggest that people at low risk of developing type 2 diabetes over the next ten years have a healthier lifestyle and better health promotion behaviors than those who are more at risk. Chen (21) and Lin (29) found that people with a healthier lifestyle are less at risk for metabolic syndrome. In Ghanei's study, lifestyle modification and promotion led to a decrease in the incidence of type 2 diabetes in samples that confirmed the association of lifestyle with diabetes (30). Wu in his study found that the healthy participants compared to those with metabolic syndrome had a better mean score in some dimensions of health promotion behaviors but there was not a significant difference between the two groups (22). There was no significant relationship between the health promotion behaviors and its dimensions with the risk of type 2 diabetes in the Sutherland’s study, which the differences in the results were probably due to the type of research and the used tool and the difference in the samples (12).
Conclusion
The results of this study show that women have a moderate level of health-promoting behaviors. According to the findings of this study, there is a significant difference in the relationship between the dimensions of health promotion behaviors and the severity of the risk of type 2 diabetes in at-risk groups. Therefore, the high-risk and very high-risk groups have fewer health-promoting behaviors than low-risk and very low-risk groups of type 2 diabetes. In other words, people with a healthier lifestyle are less likely to develop type 2 diabetes. In addition, this study refers to the role of health-promoting behaviors in the development of type 2 diabetes and emphasizes planning for community health promotion, especially for women, by policymakers. The lowest mean score and the most significant measure in the dimensions of health-promoting behaviors are associated with exercise in all five risk groups for type 2 diabetes, which indicates that physical inactivity is a strong risk factor for pre-diabetes and diabetes and represents the current lifestyle of people. Hence, health policymakers should focus their programs on removing barriers to physical activity, especially for women. In addition, more attention should be paid to improving the physical activity status of the identified high-risk and very high-risk groups of type 2 diabetes.Considering the prevention/treatment approach and the need to identify those at risk for type 2 diabetes, we used FIND RISK in which through individual clinical information, the odds of developing type 2 diabetes over the next ten years will be assessed. This method is non-invasive and cost-effective and is widely used in the community.
The limitations of the present study are collecting data by self-reporting and not observing health promotion behaviors and mental states of the samples when answering questions. Most women referring to the community health centers have a suckling child and this leads to restrictions on the regular physical activity of mothers. Therefore, the results of this study cannot be generalized to all women in society. It is suggested that health promotion behaviors be examined in a larger society of women and in direct observation of their long-term behavior.
Acknowledgements
The present article is presented in the form of a student thesis with the ethics code of IR.GUMS.REC.1395.163, sponsored by the Research Center for Social Factors Affecting Health of Guilan University of Medical Sciences. We are grateful to the respectable authorities of the community health centers of Rasht and the participants of the study who were cooperating in the implementation of this research.
Full-Text: (1388 Views)
Abstract
Background and objectives: Diabetes is the most common metabolic disease in developing countries. Because the cause of many chronic diseases lies in the human's lifestyle, performing health promotion behaviors is the best way to maintain and improve the health. Hence, this study aimed to compare the health promoting behaviors based on the Pender model in at risk groups of type 2 diabetes in women referred to health centers of Rasht city 2017.
Methods: This cross-sectional and analytical-descriptive study was performed on 300 women referring to community health centers of Rasht city and was conducted by stratified random sampling method. Data was collected by Health-Promoting Lifestyle Profile-II (HPLP-II) Questionnaire and the questionnaire evaluating the risk of type 2 diabetes using the FINDRISK tool .Data analysis was performed by SPSS version 21 using ANOVA test, Tukey test and independent T-test.
Results: The mean score and standard deviation of health promotion behaviors in this study have been varied from 144.18 ± 19.56 in the low risk group and 129.27±17.86 in the very high-risk group of type 2 diabetes. The difference in score of health promotion behaviors dimensions in the five groups according to the risk of type 2 diabetes, except the interpersonal relationships dimension, was statistically significant (P< 0.05).
Conclusion: The high risk and very high risk groups than low risk and very low risk of type 2 diabetes had less scores of health promoting behaviors. In other words, people with a healthier lifestyle were less likely to develop type 2 diabetes .
Keywords: Type 2 Diabetes , Health Promotion Behaviors, Community health centers- Women-Rasht.
Introduction
Diabetes mellitus is the most common non-communicable metabolic diseases in the developing world (1). According to the International Federation, the incidence of diabetes in 2013 has been 382 million (8.3%) and is expected to reach 592 million (8.8%) in 2035 (2). According to the World Health Organization, the prevalence of diabetes in Iran in 2016 was 9.6% in men and 11.1% in women, and this disease is responsible for 2% of deaths (3). Type 2 diabetes involves 90-95% of all diabetes cases in the world (4). Failure to control diabetes with complications in small and large vessels causes nephropathy, retinopathy, coronary artery, and peripheral vascular disease [5].
Type 2 diabetes is called lifestyle-related diabetes. Risk factors associated with lifestyle and diabetes include unhealthy nutrition, physical inactivity, smoking, alcohol consumption, socioeconomic factors, environmental conditions, and stress. In addition, type II diabetes is a preventable condition (6). Exercise, nutrition, and having proper social behaviors have an effective role in reducing the disease (7). According to research, the cause of many chronic diseases is lifestyle. Health promotion is one of the best ways in which people can maintain their health that has a direct link to disease prevention (8). The World Health Organization (WHO) estimates that 70 to 80 percent of deaths in developed countries and 40 to 50 percent of deaths in less developed countries are related to the lack of health promotion behaviors (7). According to theorists, health-promoting behaviors have a positive impact on quality of life, and individuals with health-promoting behaviors are healthier and less likely to suffer from illness. Health promoting behaviors improve quality of life and prevent and treat diseases (9). Pender's health promotion model is one of the nursing descriptive models that anticipate health behaviors, giving nurses more opportunities to explore families and communities in order to improve health and quality of life (10). Leo et al. (2006) found that although middle-aged people are at increased risk for metabolic diseases, they have a moderate level of health-promoting behaviors (11). In the Sutherland study that examined the health promotion lifestyle based on the risk of diabetes, there was no statistically significant difference between the dimensions of health-promoting behaviors and the risk of type 2 diabetes (12). The health system approach to protecting and promoting health and preventing non-communicable diseases and reducing costs on the one hand, and the growing trend of diabetes, especially in women, on the other hand, highlights the importance of promoting women's health. Despite studies on diabetes, there is still room for research on the study of risk factors for diabetes and its related health promotion behaviors in Guilan province, especially among women. The question is whether health-promoting behaviors based on the Pender model are different in women at very low risk to very high levels of type 2 diabetes. Therefore, the researcher is seeking to compare the health promoting behaviors in the at-risk groups of type 2 diabetes in women referring to community health centers in Rasht. It is hoped that the findings of this study will be a step forward in promoting women's health.
Materials and Methods
The present study is a descriptive-analytic cross-sectional study. The research populations are all community health centers of Rasht city. The samples were selected from all women referred to public health centers in Rasht via stratified random sampling (with proportional allocation). The criteria for entering the study include informed and written consent, over 18 years of age, no diagnosis of diabetes (type I and II), lack of sensory-motor limitation, cognitive impairment, and mental illness, and no pregnancy as reported by the samples. Since the data were collected in a cross-sectional fashion in one-step, the exclusion criteria were not considered.
The sample size of the study was specified based on the results of Sutherland et al. With 95% confidence, 80% Test power, 60 cases for each type 2 diabetes risk group, and a total of 300 patients to examine the significant statistical difference of samples.
A tool for collecting data in this study was a three-part questionnaire. The first part of the questionnaire was personal-social information (age, education, marital status, occupation, number of household members, monthly income of the family, and satisfaction with monthly income), the second part of the standard questionnaire of health promotion lifestyle profile 2 (HPLP2), which was developed by Walker et al. was designed based on Pender’s model. The questionnaire includes 52 items that measure six dimensions of health-promoting behaviors. These six dimensions are nutrition with 9 questions, exercise with 8 questions, responsibility for health with 9 questions, stress management with 8 questions, interpersonal support with 9 questions, and self-actualization with 9 questions.
The scoring scale in each area is based on the Likert scale in the range of "never" with the score of 1 and "always" with the score of 4, in which, scores higher than the mean represents the better status of health-promoting behaviors. So that the range of scores would be from 52 to 208 (13). The reliability and validity of the tool have been approved in various cultures and communities. Hosseini et al. (2012) also performed the psychometric verification of this tool in the Persian language. The validity of the tool was confirmed by the construct content validity method and its reliability was confirmed by test-retest method (r = 0.92) and internal consistency (Cronbach's alpha = 0.95 = α) (14). The third part of the type 2 diabetes risk assessment tool is based on the FINDRISC (Finish type2 diabetes risk score) tool. The questionnaire consists of eight questions that identify the odds of diabetes in person over the next 10 years. With the score of this tool, people were classified in five groups at risk for diabetes as very low risk (score below 7), low risk (7-11points), medium risk (12-14 points), high risk (15-20 points), and very high risk (more than 20 points) (15). Since the content of this tool does not evaluate people's views on social, cultural and religious issues, content validity and reliability have not been determined. In this questionnaire, only one option for measuring waist circumference based on the anthropometric characteristics of Iranian women included in the national program, and then localized and reset (16).
Researcher after obtaining a written letter of permission from Research Center for Social Factors Affecting Health and Deputy of Research and Technology of Guilan University of Medical Sciences visited the urban community health centers to collect data, after introducing the research objectives and coordinating with the community health centers. In this study, five groups (from low risk to high risk of diabetes) were considered as five categories. All health centers in Rasht city (16 centers) were selected as the research population. The total number of selected samples from each community health center was determined according to the visitors of that center (according to the statistics of last month's visitors), and the sampling continued until the completion of the number of samples in each of the five categories mentioned above. Four hundred people were interviewed and then, Up to 300 people with research criteria entered the study. Data collection was done through a self-report questionnaire and a part that determined the risk level of type 2 diabetes (FIND RISC tool) was evaluated by the researcher himself. Individuals were categorized according to the risk level of diabetes, and the lifestyle questionnaire was completed by the samples themselves. In non-literate participants, both parts of the questionnaire were completed by the researcher through the interview. Data was analyzed by SPSS software version 21 using ANOVA and chi-square statistical tests. Based on the KS test, the normality of the health-promoting behaviors scores followed a normal distribution.
Results:
The mean age of the participants was 39.39 ± 9.66. The majority of them were married (87.3%) with four family members (39.3%), diploma education (34%), under diploma[1] (without diploma) (32%), and university education (31.7%). In addition, the majority of the participants were homemaker (72%) and their monthly income was more than ten million Rials (54.3%) and 60.3% of them were dissatisfied with their income.
In total, 63% of the samples had a mean score of health-promoting behavior of above 130 and 37% of them had a mean score of below 130. The Scores higher and lower than the mean score (130) indicate desirable and undesirable health-promoting behaviors, respectively. The highest percentage of the desirable condition, was related to very low-risk, low- risk, and medium-risk groups, and lowest percentage of the favorable condition, was related to very high-risk group (46.7%) and it is statistically significant (p = 0.02) (Table 1).
The total mean scores of health-promoting behaviors in the five groups in terms of the risk of type 2 diabetes from the very low to very high-risk groups are, respectively, 141.48 ± 22.16, 144.18 ± 19.56, 136.93 ± 17.03, 131.15 ± 18.19, and 129.27 ± 17.86. This indicates a decrease in the mean score of health promotion behaviors from a very low-risk group to a very high-risk for type 2 diabetes.
In measuring the dimensions of health promotion behaviors, the highest score was related to the self-actualization in the low-risk group with the mean and standard deviation of 28.8 ± 4.43 and the lowest score was related to the exercise dimension in the very high-risk group with the mean and standard deviation of 11.68 ± 4.71.
Based on the results (Table 2), except for the interpersonal support score, the difference in the score of other dimensions of health promotion behaviors was statistically significant in terms of the risk groups of type 2 diabetes (p <0.05). The comparison of the mean scores of the dimensions of health-promoting behaviors in the five risk groups of type 2 diabetes indicates that the highest mean scores are observed, respectively , in self-actualization (28.80 ± 4.43), health accountability (26.02 ± 5.13), interpersonal support ( 27.33 ± 4.37), and stress management (20.67 ± 4.05) dimensions in the low-risk group of type II diabetes. The highest mean scores in exercise (16.35 ± 6.27) and nutrition (25.74 ± 4.10) dimensions are observed in the very low-risk group of type II diabetes.
Comparing the total mean score of health-promoting behaviors in the five risk groups of type 2 diabetes, the highest score (144.18 ± 19.56) belonged to the low-risk group and the lowest score (129.27 ± 17.86) belonged to the very high-risk group Which was statistically significant (p = 0.0001).
Table1-Frequency of health promotion behaviors (desirable and undesirable) Depending on the risk of type 2 diabetes in the sample
Background and objectives: Diabetes is the most common metabolic disease in developing countries. Because the cause of many chronic diseases lies in the human's lifestyle, performing health promotion behaviors is the best way to maintain and improve the health. Hence, this study aimed to compare the health promoting behaviors based on the Pender model in at risk groups of type 2 diabetes in women referred to health centers of Rasht city 2017.
Methods: This cross-sectional and analytical-descriptive study was performed on 300 women referring to community health centers of Rasht city and was conducted by stratified random sampling method. Data was collected by Health-Promoting Lifestyle Profile-II (HPLP-II) Questionnaire and the questionnaire evaluating the risk of type 2 diabetes using the FINDRISK tool .Data analysis was performed by SPSS version 21 using ANOVA test, Tukey test and independent T-test.
Results: The mean score and standard deviation of health promotion behaviors in this study have been varied from 144.18 ± 19.56 in the low risk group and 129.27±17.86 in the very high-risk group of type 2 diabetes. The difference in score of health promotion behaviors dimensions in the five groups according to the risk of type 2 diabetes, except the interpersonal relationships dimension, was statistically significant (P< 0.05).
Conclusion: The high risk and very high risk groups than low risk and very low risk of type 2 diabetes had less scores of health promoting behaviors. In other words, people with a healthier lifestyle were less likely to develop type 2 diabetes .
Keywords: Type 2 Diabetes , Health Promotion Behaviors, Community health centers- Women-Rasht.
Introduction
Diabetes mellitus is the most common non-communicable metabolic diseases in the developing world (1). According to the International Federation, the incidence of diabetes in 2013 has been 382 million (8.3%) and is expected to reach 592 million (8.8%) in 2035 (2). According to the World Health Organization, the prevalence of diabetes in Iran in 2016 was 9.6% in men and 11.1% in women, and this disease is responsible for 2% of deaths (3). Type 2 diabetes involves 90-95% of all diabetes cases in the world (4). Failure to control diabetes with complications in small and large vessels causes nephropathy, retinopathy, coronary artery, and peripheral vascular disease [5].
Type 2 diabetes is called lifestyle-related diabetes. Risk factors associated with lifestyle and diabetes include unhealthy nutrition, physical inactivity, smoking, alcohol consumption, socioeconomic factors, environmental conditions, and stress. In addition, type II diabetes is a preventable condition (6). Exercise, nutrition, and having proper social behaviors have an effective role in reducing the disease (7). According to research, the cause of many chronic diseases is lifestyle. Health promotion is one of the best ways in which people can maintain their health that has a direct link to disease prevention (8). The World Health Organization (WHO) estimates that 70 to 80 percent of deaths in developed countries and 40 to 50 percent of deaths in less developed countries are related to the lack of health promotion behaviors (7). According to theorists, health-promoting behaviors have a positive impact on quality of life, and individuals with health-promoting behaviors are healthier and less likely to suffer from illness. Health promoting behaviors improve quality of life and prevent and treat diseases (9). Pender's health promotion model is one of the nursing descriptive models that anticipate health behaviors, giving nurses more opportunities to explore families and communities in order to improve health and quality of life (10). Leo et al. (2006) found that although middle-aged people are at increased risk for metabolic diseases, they have a moderate level of health-promoting behaviors (11). In the Sutherland study that examined the health promotion lifestyle based on the risk of diabetes, there was no statistically significant difference between the dimensions of health-promoting behaviors and the risk of type 2 diabetes (12). The health system approach to protecting and promoting health and preventing non-communicable diseases and reducing costs on the one hand, and the growing trend of diabetes, especially in women, on the other hand, highlights the importance of promoting women's health. Despite studies on diabetes, there is still room for research on the study of risk factors for diabetes and its related health promotion behaviors in Guilan province, especially among women. The question is whether health-promoting behaviors based on the Pender model are different in women at very low risk to very high levels of type 2 diabetes. Therefore, the researcher is seeking to compare the health promoting behaviors in the at-risk groups of type 2 diabetes in women referring to community health centers in Rasht. It is hoped that the findings of this study will be a step forward in promoting women's health.
Materials and Methods
The present study is a descriptive-analytic cross-sectional study. The research populations are all community health centers of Rasht city. The samples were selected from all women referred to public health centers in Rasht via stratified random sampling (with proportional allocation). The criteria for entering the study include informed and written consent, over 18 years of age, no diagnosis of diabetes (type I and II), lack of sensory-motor limitation, cognitive impairment, and mental illness, and no pregnancy as reported by the samples. Since the data were collected in a cross-sectional fashion in one-step, the exclusion criteria were not considered.
The sample size of the study was specified based on the results of Sutherland et al. With 95% confidence, 80% Test power, 60 cases for each type 2 diabetes risk group, and a total of 300 patients to examine the significant statistical difference of samples.
A tool for collecting data in this study was a three-part questionnaire. The first part of the questionnaire was personal-social information (age, education, marital status, occupation, number of household members, monthly income of the family, and satisfaction with monthly income), the second part of the standard questionnaire of health promotion lifestyle profile 2 (HPLP2), which was developed by Walker et al. was designed based on Pender’s model. The questionnaire includes 52 items that measure six dimensions of health-promoting behaviors. These six dimensions are nutrition with 9 questions, exercise with 8 questions, responsibility for health with 9 questions, stress management with 8 questions, interpersonal support with 9 questions, and self-actualization with 9 questions.
The scoring scale in each area is based on the Likert scale in the range of "never" with the score of 1 and "always" with the score of 4, in which, scores higher than the mean represents the better status of health-promoting behaviors. So that the range of scores would be from 52 to 208 (13). The reliability and validity of the tool have been approved in various cultures and communities. Hosseini et al. (2012) also performed the psychometric verification of this tool in the Persian language. The validity of the tool was confirmed by the construct content validity method and its reliability was confirmed by test-retest method (r = 0.92) and internal consistency (Cronbach's alpha = 0.95 = α) (14). The third part of the type 2 diabetes risk assessment tool is based on the FINDRISC (Finish type2 diabetes risk score) tool. The questionnaire consists of eight questions that identify the odds of diabetes in person over the next 10 years. With the score of this tool, people were classified in five groups at risk for diabetes as very low risk (score below 7), low risk (7-11points), medium risk (12-14 points), high risk (15-20 points), and very high risk (more than 20 points) (15). Since the content of this tool does not evaluate people's views on social, cultural and religious issues, content validity and reliability have not been determined. In this questionnaire, only one option for measuring waist circumference based on the anthropometric characteristics of Iranian women included in the national program, and then localized and reset (16).
Researcher after obtaining a written letter of permission from Research Center for Social Factors Affecting Health and Deputy of Research and Technology of Guilan University of Medical Sciences visited the urban community health centers to collect data, after introducing the research objectives and coordinating with the community health centers. In this study, five groups (from low risk to high risk of diabetes) were considered as five categories. All health centers in Rasht city (16 centers) were selected as the research population. The total number of selected samples from each community health center was determined according to the visitors of that center (according to the statistics of last month's visitors), and the sampling continued until the completion of the number of samples in each of the five categories mentioned above. Four hundred people were interviewed and then, Up to 300 people with research criteria entered the study. Data collection was done through a self-report questionnaire and a part that determined the risk level of type 2 diabetes (FIND RISC tool) was evaluated by the researcher himself. Individuals were categorized according to the risk level of diabetes, and the lifestyle questionnaire was completed by the samples themselves. In non-literate participants, both parts of the questionnaire were completed by the researcher through the interview. Data was analyzed by SPSS software version 21 using ANOVA and chi-square statistical tests. Based on the KS test, the normality of the health-promoting behaviors scores followed a normal distribution.
Results:
The mean age of the participants was 39.39 ± 9.66. The majority of them were married (87.3%) with four family members (39.3%), diploma education (34%), under diploma[1] (without diploma) (32%), and university education (31.7%). In addition, the majority of the participants were homemaker (72%) and their monthly income was more than ten million Rials (54.3%) and 60.3% of them were dissatisfied with their income.
In total, 63% of the samples had a mean score of health-promoting behavior of above 130 and 37% of them had a mean score of below 130. The Scores higher and lower than the mean score (130) indicate desirable and undesirable health-promoting behaviors, respectively. The highest percentage of the desirable condition, was related to very low-risk, low- risk, and medium-risk groups, and lowest percentage of the favorable condition, was related to very high-risk group (46.7%) and it is statistically significant (p = 0.02) (Table 1).
The total mean scores of health-promoting behaviors in the five groups in terms of the risk of type 2 diabetes from the very low to very high-risk groups are, respectively, 141.48 ± 22.16, 144.18 ± 19.56, 136.93 ± 17.03, 131.15 ± 18.19, and 129.27 ± 17.86. This indicates a decrease in the mean score of health promotion behaviors from a very low-risk group to a very high-risk for type 2 diabetes.
In measuring the dimensions of health promotion behaviors, the highest score was related to the self-actualization in the low-risk group with the mean and standard deviation of 28.8 ± 4.43 and the lowest score was related to the exercise dimension in the very high-risk group with the mean and standard deviation of 11.68 ± 4.71.
Based on the results (Table 2), except for the interpersonal support score, the difference in the score of other dimensions of health promotion behaviors was statistically significant in terms of the risk groups of type 2 diabetes (p <0.05). The comparison of the mean scores of the dimensions of health-promoting behaviors in the five risk groups of type 2 diabetes indicates that the highest mean scores are observed, respectively , in self-actualization (28.80 ± 4.43), health accountability (26.02 ± 5.13), interpersonal support ( 27.33 ± 4.37), and stress management (20.67 ± 4.05) dimensions in the low-risk group of type II diabetes. The highest mean scores in exercise (16.35 ± 6.27) and nutrition (25.74 ± 4.10) dimensions are observed in the very low-risk group of type II diabetes.
Comparing the total mean score of health-promoting behaviors in the five risk groups of type 2 diabetes, the highest score (144.18 ± 19.56) belonged to the low-risk group and the lowest score (129.27 ± 17.86) belonged to the very high-risk group Which was statistically significant (p = 0.0001).
Table1-Frequency of health promotion behaviors (desirable and undesirable) Depending on the risk of type 2 diabetes in the sample
| The status of health promoting behaviors The risk of diabetese |
Undesirable Percent / number |
desirable Percent / number |
total | p* | |
| Very low risk |
The number / percentage of people at risk for type 2 diabetes |
18(%30) | 42(%70) | 60(%100) |
0.02
|
| low risk | The number / percentage of people at risk for type 2 diabetes |
18(%30) | 42(%70) | 60(%100) |
|
| Medium risk | The number / percentage of people at risk for type 2 diabetes |
18(%30) | 42(%70) | 60(%100) |
|
| High risk | The number / percentage of people at risk for type 2 diabetes |
25(%41/7) | 35(%58.3) | 60(%100) |
|
| Very High risk | The number / percentage of people at risk for type 2 diabetes |
32(%53.3) | 28(%46.7) | 60(%100) |
|
| total | The number / percentage of people at risk for type 2 diabetes |
111(%37) | 189(%63) | 300(%100) | |
Table 2- The mean and standard deviation of the dimensions of health promotion behaviors in the groups at risk for type 2 diabetes in the studied samples
| Dimensions of health promotion behaviors |
The risk of developing type 2 diabetes |
||||||
| Very low risk |
Low risk |
Medium risk |
High risk |
Very high risk |
P* | ||
| Spiritual Growth | Mean | 27.38 | 28.80 | 26.85 | 26.95 | 26.15 | 0.024 |
| Standard Deviation | 4.46 | 4.43 | 4.49 | 4.45 | 4.07 | ||
| Health Responsibility | Mean | 25.77 | 26.02 | 25.63 | 23.43 | 23.58 | 0.009 |
| Standard Deviation | 5.68 | 5.13 | 4.87 | 4.93 | 5.54 | ||
| Interpersonal Relationship | Mean | 26.45 | 27.33 | 25.73 | 25.28 | 25.72 | 0.119 |
| Standard Deviation | 4.93 | 4.37 | 4.36 | 4.58 | 4.63 | ||
| Stress Management | Mean | 19.82 | 20.67 | 18.93 | 19.28 | 18.25 | 0.011 |
| Standard Deviation | 4.45 | 4.05 | 3.55 | 3.62 | 3.68 | ||
| Physical Activity | Mean | 16.35 | 15.70 | 14.33 | 12.43 | 11.68 | 0.0001 |
| Standard Deviation | 6.27 | 6.13 | 4.85 | 4.49 | 4.71 | ||
| Nutrition | Mean | 25.72 | 25.67 | 25.45 | 23.75 | 23.88 | 0.003 |
| Standard Deviation | 4.10 | 3.84 | 3.56 | 3.69 | 3.89 | ||
| Total | Mean | 141.48 | 144.18 | 136.93 | 131.15 | 129.27 | 0.0001 |
| Standard Deviation | 22.16 | 19.56 | 17.03 | 18.19 | 17.86 | ||
Diagram 1: Average Score of Health Promotion Behavioral Dimensions In groups at risk for type 2 diabetese
Discussion
The women of this study showed a moderate level of health-promoting behaviors. In a large number of studies that examined the health-promoting behaviors in the women's population, similar results were obtained (17), (18), (19), and (20). Women's health should be an important aspect of advancement in societies and health policies, and policymakers and health providers should plan and intervene to promote health in this target group. The total mean score of health-promoting behaviors in the five groups at risk for type 2 diabetes was different so that the lowest and highest risk groups received the lowest score. Compared to the five groups, this difference was statistically significant, which indicates that the status of the health-promoting behaviors in the low-risk group is desirable but in the high-risk group of type II diabetes is undesirable. In Chen's study, people at risk for metabolic syndrome had better health-promoting behaviors than those with metabolic syndrome (21). In addition, in the Wu’s study, in general, the samples showed a moderate level of health-promoting behaviors, and the healthy participants had higher levels of health-promoting behaviors than those with metabolic syndrome (22). El mokadem in his study found that there was a statistically significant difference between the score of health-promoting behaviors and the risk score for cardiovascular disease (diabetes and hypertension) in women (23). However, Sutherland who examined the health-promoting behaviors with regard to the risk of diabetes found that the average score of health-promoting behaviors in the natural group was lower than the diabetic group (12). Furthermore, in Sorour's study, there was no significant relationship between the mean score of health-promoting behaviors and chronic illnesses (24). Differences in results may be related to the type of research and tools used and the difference in the research samples.
The results indicate that there is a relationship between women's health-promoting behaviors and their risk of developing type 2 diabetes over the next ten years (26). More attention of policy makers and health service providers is essential for promoting women's health as one of the major dimensions of community development. Findings of the research regarding the dimensions of health-promoting behaviors indicate that the highest mean score in self-actualization dimension is in line with many similar studies (18), (12), and (26). Self-actualization, which is a psychological factor influencing the realization of the potential ability of individuals to "get the best", is a health-promoting factor (17). The Iranian women's religion is an influential factor in self-actualization. In the review of different studies, there was a difference in dimensions that had the highest average score due to differences in cultures and factors influencing health-promotion behaviors and the different units of the research. However, in most studies, the highest mean score is related to self-actualization and interpersonal relationships influenced by culture and religion. In most studies, the lowest mean score was related to exercise. The result was consistent with the results of some studies (27), (12), (26), (21) which could be related to the industrial lifestyle. This kind of lifestyle has become a problem for many countries because the positive impact of physical activity on health is undeniable. Physical inactivity is a major risk factor for pre-diabetes. Physical activity is essential for women and physical inactivity makes them susceptible to cardiovascular disease and diabetes (28).
Based on the findings, except for the mean score of interpersonal support, the scores of other dimensions in terms of the risk groups of type 2 diabetes were statistically significant. The score of health-promoting behaviors in all studied areas has a descending trend from low-risk and very low-risk groups to high-risk and very high-risk groups. These findings suggest that people at low risk of developing type 2 diabetes over the next ten years have a healthier lifestyle and better health promotion behaviors than those who are more at risk. Chen (21) and Lin (29) found that people with a healthier lifestyle are less at risk for metabolic syndrome. In Ghanei's study, lifestyle modification and promotion led to a decrease in the incidence of type 2 diabetes in samples that confirmed the association of lifestyle with diabetes (30). Wu in his study found that the healthy participants compared to those with metabolic syndrome had a better mean score in some dimensions of health promotion behaviors but there was not a significant difference between the two groups (22). There was no significant relationship between the health promotion behaviors and its dimensions with the risk of type 2 diabetes in the Sutherland’s study, which the differences in the results were probably due to the type of research and the used tool and the difference in the samples (12).
Conclusion
The results of this study show that women have a moderate level of health-promoting behaviors. According to the findings of this study, there is a significant difference in the relationship between the dimensions of health promotion behaviors and the severity of the risk of type 2 diabetes in at-risk groups. Therefore, the high-risk and very high-risk groups have fewer health-promoting behaviors than low-risk and very low-risk groups of type 2 diabetes. In other words, people with a healthier lifestyle are less likely to develop type 2 diabetes. In addition, this study refers to the role of health-promoting behaviors in the development of type 2 diabetes and emphasizes planning for community health promotion, especially for women, by policymakers. The lowest mean score and the most significant measure in the dimensions of health-promoting behaviors are associated with exercise in all five risk groups for type 2 diabetes, which indicates that physical inactivity is a strong risk factor for pre-diabetes and diabetes and represents the current lifestyle of people. Hence, health policymakers should focus their programs on removing barriers to physical activity, especially for women. In addition, more attention should be paid to improving the physical activity status of the identified high-risk and very high-risk groups of type 2 diabetes.Considering the prevention/treatment approach and the need to identify those at risk for type 2 diabetes, we used FIND RISK in which through individual clinical information, the odds of developing type 2 diabetes over the next ten years will be assessed. This method is non-invasive and cost-effective and is widely used in the community.
The limitations of the present study are collecting data by self-reporting and not observing health promotion behaviors and mental states of the samples when answering questions. Most women referring to the community health centers have a suckling child and this leads to restrictions on the regular physical activity of mothers. Therefore, the results of this study cannot be generalized to all women in society. It is suggested that health promotion behaviors be examined in a larger society of women and in direct observation of their long-term behavior.
Acknowledgements
The present article is presented in the form of a student thesis with the ethics code of IR.GUMS.REC.1395.163, sponsored by the Research Center for Social Factors Affecting Health of Guilan University of Medical Sciences. We are grateful to the respectable authorities of the community health centers of Rasht and the participants of the study who were cooperating in the implementation of this research.
Type of study: Original Article |
References
1. Shakeri MT, Rasulian A, Erfanian Taphvaee MR, Etemad Rezaee SH, Emadzadeh M. Evaluation of relation ship between anthropometric indexes and diabetes. Medical Journal of Mashhad University of Medical Sciences. 2015;58(7):390-6 [persian]. [Google Scholar]
2. Pham NM, Eggleston K. Prevalence and determinants of diabetes and prediabetes among Vietnamese adults. Diabetes Research And Clinical Practice. 2016;113:116-24. [DOI:10.1016/j.diabres.2015.12.009] [Google Scholar]
3. World Health Organization - Diabetes country profiles, 2016 Available at: http://www.who.int/diabetes/country-profiles/en/.
4. Li R, Qu S, Zhang P, Chattopadhyay S, Gregg EW, Albright A, et al. Economic evaluation of combined diet and physical activity promotion programs to prevent type 2 diabetes among persons at increased risk: a systematic review for the community preventive services task force. Annals of internal medicine. 2015;163(6):452-60. [DOI:10.7326/M15-0469]
5. Beagley J, Guariguata L, Weil C, Motala AA. Global estimates of undiagnosed diabetes in adults. Diabetes Research And Clinical Practice. 2014;103(2):150-60. [DOI:10.1016/j.diabres.2013.11.001] [Google Scholar]
6. Momeni Javid F, Simbar M, Dolatian M, Alavi Majd H. Comparison of pregnancy self-care, perceived social support and perceived stress of women with gestational diabetes and healthy pregnant women. Iranian Journal Of Endocrinology And Metabolism. 2014;16(3):156-64 [persian]. [DOI:10.5539/gjhs.v7n2p162] [Google Scholar]
7. Kalroozi F, Pishgooie AH, Taheriyan A. Health-promoting behaviours in employed nurses in selected military Hospitals. Journal Of Health Promotion Management. 2015;4(2):7-15 [persian]. [DOI:10.18869/acadpub.mcs.1.2.73] [Google Scholar]
8. Rashedi S, Bahrami M. Factors related to the health promoting life style among geriatric patients. Journal Of Urmia Nursing And Midwifery Faculty. 2015;13(2):90-8 [persian]. [Google Scholar]
9. mohaddesi H, razavi S R, Khalkhali H R, bahadori F, saeigharenaz M. The effect of counseling on health promotion behaviors in diabetic mothers referred to motahhari hospital of urmia at 2015. Journal of Urmia Nursing And Midwifery Faculty. 2016;14(9):757-66 [persian]. [Google Scholar]
10. Radmehr M, Ashktorab T, Neisi L. Effect of the educational program based on Pender's theory on the health promotion in patients with obsessive-compulsive disorder. Journal of Nursing Education. 2013;2(2):56-63 [persian]. [Google Scholar]
11. Lo SWS, Chair SY, Lee FK. Factors associated with health-promoting behavior of people with or at high risk of metabolic syndrome: Based on the health belief model. Applied Nursing Research. 2015;28(2):197-201. [DOI:10.1016/j.apnr.2014.11.001] [Google Scholar]
12. Sutherland LL, Weiler DM, Bond L, Simonson S, Reis J. Northwest Latinos' health promotion lifestyle profiles according to diabetes risk status. Journal Of Immigrant And Minority Health. 2012;14(6):999-1005. [DOI:10.1007/s10903-012-9641-3] [Google Scholar]
13. Mahmoodi H, Asghari Jafarabadi M, Mohammadi Y, Shirzadi S, Sadeghi M, Sharifisaqezi P. Correlation of body mass index and health-promoting lifestyle among health care workers of saqqez city. Journal Of Health Promotion Management. 2016;5(2):42-51 [persian]. [Google Scholar]
14. rastegar m, zendehtalab h, mazlom s, yavari m. Effect of peer education on health promoting lifestyle among volunteer health care communicators. Journal of Nursing Education. 2017;6(2):9-17 [persian]. [DOI:10.21859/jne-06022] [Google Scholar]
15. García-Alcalá H, Genestier-Tamborero CN, Hirales-Tamez O, Salinas-Palma J, Soto-Vega E. Frequency of diabetes, impaired fasting glucose, and glucose intolerance in high-risk groups identified by a FINDRISC survey in Puebla City, Mexico. Diabetes, Metabolic Syndrome And Obesity: Targets And Therapy. 2012;5:403. [DOI:10.2147/DMSO.S35545] [Google Scholar]
16. Mardani M, Rafiee E, Ebrahimzadeh F, Baba H, Balavar S, Alimohamadi M. Prevalence of metabolic syndrome among students of Lorestan University of Medical Sciences during 2011-2012. Medical Journal Of Mashhad University Of Medical Sciences. 2015;57(8):918-25. [persian] [Google Scholar]
17. Bakouei S, Bakouei F, Omidvar S, Bakhtiari A. Health-promoting behaviors and their predictors in iranian women of reproductive age: a cross-sectional study. International Quarterly Of Community Health Education.2017;38(1):3-8 [persian]. [DOI:10.1177/0272684X17747053] [Google Scholar]
18. Kirag N, Ocaktan EM. Analysis of health promoting lifestyle behaviors and associated factors among nurses at a university hospital in Turkey. Saudi Med J. 2013;34(10):1062-7. [Google Scholar]
19. Asrami FS, Hamzehgardeshi Z, Shahhosseini Z. Health promoting lifestyle behaviors in menopausal women: A Cross-Sectional Study. Global Journal Of Health Science. 2016;8(8):128-134 [persian]. [DOI:10.5539/gjhs.v8n8p128] [Google Scholar]
20. Sonmezer H, Cetinkaya F, Nacar M. Healthy life-style promoting behaviour in Turkish women aged 18-64. Asian Pac J Cancer Prev. 2012;13(4):1241-5. [DOI:10.7314/APJCP.2012.13.4.1241] [Google Scholar]
21. Chen YC, Wu HP, Hwang SJ, Li I-C. Exploring the components of metabolic syndrome with respect to gender difference and its relationship to health‐promoting lifestyle behaviour: a study in Taiwanese urban communities. Journal Of Clinical Nursing. 2010;19(21‐22):3031-41. [DOI:10.1111/j.1365-2702.2010.03280.x] [Google Scholar]
22. Wu T-T, Chen I-J, Cho S-L, Chiou A-F. The relationship between health-promoting behaviors and metabolic syndrome in community-dwelling older adults. Biological Research For Nursing. 2016;18(5):549-57. [DOI:10.1177/1099800416655882] [Google Scholar]
23. Elmokadem NM. Health promoting lifestyle behaviors among women at high risk for cardiovascular diseases. The Medical Journal of Cairo University. 2013;81(2):83-88 [Google Scholar]
24. Sorour AS, Kamel WW, El-Aziz EMA, Aboelseoud A. Health promoting lifestyle behaviors and related risk factors among female employees in Zagazig city. Journal of Nursing Education and Practice. 2014;4(5):42. [DOI:10.5430/jnep.v4n5p42] [Google Scholar]
25. Tuso P. Prediabetes and lifestyle modification: time to prevent a preventable disease. The Permanente Journal. 2014;18(3):88-93. [DOI:10.7812/TPP/14-002] [Google Scholar]
26. Dutta M, Kaur H. Status of health promoting behaviours among urban females. Indian Journal Of Health And Wellbeing. 2014;5(2):195. [Google Scholar]
27. Mirghafourvand M, Baheiraei A, Nedjat S, Mohammadi E, Charandabi SM-A, Majdzadeh R. A population-based study of health-promoting behaviors and their predictors in Iranian women of reproductive age. Health Promotion International. 2014;30(3):586-94 [persian]. [DOI:10.1093/heapro/dat086] [Google Scholar]
28. Hosseinnejad M, klantarzadeh M. Lifestyle among students of islamicazad university, kerman branch based on the pender's health promotion model. Journal Of Health Education And Health Promotion.2014 ;1(4):15-28 [persian]. [Google Scholar]
29. Lin KM, Chiou JY, Ko SH, Tan JY, Huang CN, Liao WC. Modifiable lifestyle behaviors are associated with metabolic syndrome in a Taiwanese population. Journal Of Nursing Scholarship. 2015;47(6):487-95. [DOI:10.1111/jnu.12163] [Google Scholar]
30. GHaneei L, Harati H, Hadayegh F, Azizi F. The effect of life style modification on the occurrence of diabetes type 2 in a 3.5-year study: Tehran lipid and glucose study. Research in Medicine. 2009;33(1):21-29 [persian]. [Google Scholar]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
