
Volume 18, Issue 2 (7-2021)
J Res Dev Nurs Midw 2021, 18(2): 26-28 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ziaei T, Gordani N, Khoori E, Tatari M, Gharahjeh S. Evaluating Correlation of General Self-Concept with Sexual Self-Concept in Infertile Women. J Res Dev Nurs Midw 2021; 18 (2) :26-28
URL: http://nmj.goums.ac.ir/article-1-1141-en.html
URL: http://nmj.goums.ac.ir/article-1-1141-en.html



1- Associate Professor, Counseling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran
2- Counseling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran ,nooshin.gordani@yahoo.com
3- Msc in Biostatistics, Golestan University of Medical Sciences, Gorgan, Iran
4- Obstetricians and Gynecology Specialist, Fellowship in Infertility, Gorgan Infertility Center, Golestan, Iran
2- Counseling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran ,
3- Msc in Biostatistics, Golestan University of Medical Sciences, Gorgan, Iran
4- Obstetricians and Gynecology Specialist, Fellowship in Infertility, Gorgan Infertility Center, Golestan, Iran
Full-Text [PDF 545 kb]
(1681 Downloads)
| Abstract (HTML) (4415 Views)
Mean age of participants was 28.88±5.14 years (range: 17-40 years). The majority of participants were married once (97.1%), homemaker (59%) and with bachelor's degrees (38.1%). In addition, most subjects were married for less than five years (Table 1).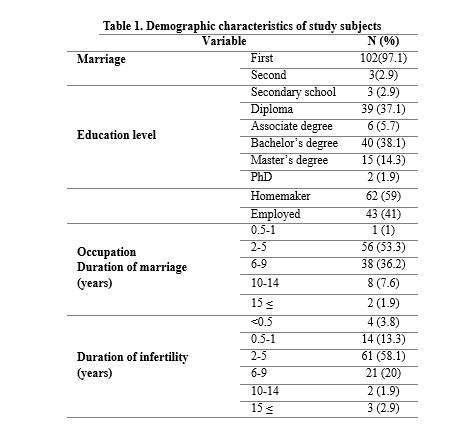
There was a statistically significant positive relationship between age and negative sexual self-concept (P=0.017, r=0.23). There was no significant correlation between age and general or positive sexual self-concept (P>0.05). The results of the Spearman's test indicated no statistically significant correlation between general self-concept and sexual self-concept in infertile women (Table 2).
Based on the results, 19% of the participants had normal general self-concept, 31.4% had moderate self-concept and 49.5% had weak self-concept. The mean scores of positive sexual self-concept, negative sexual self-concept and situational sexual self-concept were 118.9±24.85, 13.33±8.94 and 41.98± 10.53, respectively. Table 3 presents the mean score of the dimensions and subdomains of sexual self-concept.
There was no significant association between education level and self-concept scores in infertile women. The results of the Mann-Whitney test indicated a statistically significant difference in general self-concept and positive sexual self-concept scores between employed and homemaker infertile women. The results of the Kruskal-Wallis test indicated no statistically significant relationship between dimensions of sexual self-concept and the duration of the marriage or infertility.
The mean score of general self-concept, sexual self-concept and its dimensions in the levels of demographic variables such as level of education, duration of marriage, and duration of infertility were not statistically significant (P> 0.05).
There was a statistically significant difference between the mean score of general self-concept (P= 0.03) and positive sexual self-concept (P= 0.013) by occupation, but there was no statistically significant difference between the mean score of negative self-concept and position in occupation (p> 0.05)..PNG)
.PNG)
Full-Text: (1476 Views)
Highlights:
What is current knowledge?
Due to the lack of correlation between general self-concept and sexual self-concept in infertile women, evaluations and interventions on these variables can be done separately in this population.
What is new here?
There is no significant correlation between general self-concept and sexual self-concept in infertile women.
Introduction
Self-concept refers to a set of feelings and perceptions about oneself that can be acquired through social relationships and developed due to interactions with others (1). It has been considered as an important element to mental health (2). A negative self-concept manifests itself in lower self-confidence, lower performance, lack of motivation, isolation and loneliness (3), while a positive self-concept results in improved self-esteem and self-efficacy (4).
Sexual self-concept refers to individual's perception of his/her sexual feelings and actions (5, 6). This phenomenon emerges during the process of psychosocial-mental development and helps a person to achieve awareness in sexual life for self-evaluation (5). It is influenced by cognition, beliefs and environment (7) and significantly associated with sexual experiences and behaviors (8).
Snell (1995) introduced sexual self-concept in 20 dimensions (9). Ziaei et al. (2013) classified sexual self-concept into positive, negative and situational domains (10). The negative domain includes sexual anxiety, sexual depression, fear of sex and sexual monitoring (9). The positive domain consists of sexual behaviors, motivation and feelings that facilitate the growth and adaptation of self-efficient sexual beliefs that improve self-confidence and performance in sex (8). The situational domain is variable and can refer to a positive or negative concept depending on personal characteristics (10). The positive and negative dimensions of sexual self-concept are important psycho-sexual variables in life (11) that could be influenced by various life problems, such as infertility (12).
Findings indicate that infertility has a negative impact on the general self-concept of women and their attitude towards life (13). The negative attitude towards life due to not having children makes women feel a lot of responsibility towards their spouses that in turn seriously damages their self-concept (12). Karaca (2014) reported negative self-concept, social pressure, isolation and loneliness as the most important psychological problems of infertile women. In addition, insomnia, eating disorders, obsessive thoughts and symptoms of depression are some physical problems associated with infertility (13). The present study aimed to determine the correlation between self-concept and sexual self-concept in infertile women.
MethodsThis descriptive correlational study was performed on infertile women who visited the Gorgan Infertility Center in 2018. Due to the lack of a similar article to determine the sample size, we first conducted a pilot study with 30 samples, and a correlation coefficient of R=0.35 was obtained between general self-concept and positive sexual self-concept, R=0.26 between general self-concept and negative sexual self-concept, and R=0.56 between general self-concept and situational sexual self-concept. Since the greatest sample size (n= 105) was obtained with a correlation coefficient of R=0.26, 80% power and 0.95 confidence level, we considered the value as a criterion for determining the sample size.
Inclusion criteria were having Iranian nationality, at least secondary school education, no adopted children, primary infertility and no known physical or mental illness. Those who used psychiatric medications or had drug addiction were excluded from the study. Overall, 105 women were enrolled via convenience sampling. The study was approved by the ethics committee of the Golestan University of Medical Sciences (code: IR.GOUMS.REC.1397.99). After detailed explanation of the study objectives and methods, written informed consent was taken from all participants. Data were collected using a demographic characteristics form, the Rogers’ self-concept questionnaire and the Snell’s sexual self-concept questionnaire.
Rogers first introduced the self-concept questionnaire in 1951. The questionnaire consists of two forms that measure basic self-concept (form A) and ideal self-concept (form B). In both forms, there is 25 pair of contrasting personality traits, and the subject must evaluate herself/ himself according to those two traits and give herself/himself a score between 1 and 7. First, the scores obtained in forms A and B were subtracted, squared, added and then squared root to obtain the final score of an individual in the test. A total score of 0 to 7, 7.01 to 10 and 10.01 or higher indicate normal, moderate and weak self-concept, respectively. Aghajani (2008) reported the reliability coefficient of this questionnaire as 0.83 (14). Khadivi et al. (2011) verified the validity of the questionnaire by obtaining a correlation coefficient of 0.67 (15). In the present study, the reliability of the questionnaire was confirmed by obtaining a Cronbach's alpha coefficient of 0.80.
Snell (1995) first designed the sexual self-concept questionnaire for measuring individuals’ perception of sex (16). Ziaei (2013) validated the questionnaire in Iran. The Persian version of the questionnaire includes 78 items and 18 domains each of which consists of three to five items. The domains are classified into three dimensions: negative sexual self-concept, positive sexual self-concept and situational sexual self-concept. The minimum and maximum scores in the positive, negative and situational self-concept dimensions are 0-117, 0-64 and 0-77, respectively. The reliability of the questionnaire was found to be 0.76 to 0.89 (10). In the present study, the reliability of the positive, negative and situational self-concept dimensions was confirmed by obtaining Cronbach's alpha coefficient of 0.68, 0.85 and 0.73, respectively.
Data were expressed presented as mean ± standard deviation (SD). Normality of data was assessed using the Kolmogorov-Smirnov test. Data were analyzed accordingly using the Pearson's correlation coefficient and the Spearman's correlation test. SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA).
ResultsWhat is current knowledge?
Due to the lack of correlation between general self-concept and sexual self-concept in infertile women, evaluations and interventions on these variables can be done separately in this population.
What is new here?
There is no significant correlation between general self-concept and sexual self-concept in infertile women.
Introduction
Self-concept refers to a set of feelings and perceptions about oneself that can be acquired through social relationships and developed due to interactions with others (1). It has been considered as an important element to mental health (2). A negative self-concept manifests itself in lower self-confidence, lower performance, lack of motivation, isolation and loneliness (3), while a positive self-concept results in improved self-esteem and self-efficacy (4).
Sexual self-concept refers to individual's perception of his/her sexual feelings and actions (5, 6). This phenomenon emerges during the process of psychosocial-mental development and helps a person to achieve awareness in sexual life for self-evaluation (5). It is influenced by cognition, beliefs and environment (7) and significantly associated with sexual experiences and behaviors (8).
Snell (1995) introduced sexual self-concept in 20 dimensions (9). Ziaei et al. (2013) classified sexual self-concept into positive, negative and situational domains (10). The negative domain includes sexual anxiety, sexual depression, fear of sex and sexual monitoring (9). The positive domain consists of sexual behaviors, motivation and feelings that facilitate the growth and adaptation of self-efficient sexual beliefs that improve self-confidence and performance in sex (8). The situational domain is variable and can refer to a positive or negative concept depending on personal characteristics (10). The positive and negative dimensions of sexual self-concept are important psycho-sexual variables in life (11) that could be influenced by various life problems, such as infertility (12).
Findings indicate that infertility has a negative impact on the general self-concept of women and their attitude towards life (13). The negative attitude towards life due to not having children makes women feel a lot of responsibility towards their spouses that in turn seriously damages their self-concept (12). Karaca (2014) reported negative self-concept, social pressure, isolation and loneliness as the most important psychological problems of infertile women. In addition, insomnia, eating disorders, obsessive thoughts and symptoms of depression are some physical problems associated with infertility (13). The present study aimed to determine the correlation between self-concept and sexual self-concept in infertile women.
MethodsThis descriptive correlational study was performed on infertile women who visited the Gorgan Infertility Center in 2018. Due to the lack of a similar article to determine the sample size, we first conducted a pilot study with 30 samples, and a correlation coefficient of R=0.35 was obtained between general self-concept and positive sexual self-concept, R=0.26 between general self-concept and negative sexual self-concept, and R=0.56 between general self-concept and situational sexual self-concept. Since the greatest sample size (n= 105) was obtained with a correlation coefficient of R=0.26, 80% power and 0.95 confidence level, we considered the value as a criterion for determining the sample size.
Inclusion criteria were having Iranian nationality, at least secondary school education, no adopted children, primary infertility and no known physical or mental illness. Those who used psychiatric medications or had drug addiction were excluded from the study. Overall, 105 women were enrolled via convenience sampling. The study was approved by the ethics committee of the Golestan University of Medical Sciences (code: IR.GOUMS.REC.1397.99). After detailed explanation of the study objectives and methods, written informed consent was taken from all participants. Data were collected using a demographic characteristics form, the Rogers’ self-concept questionnaire and the Snell’s sexual self-concept questionnaire.
Rogers first introduced the self-concept questionnaire in 1951. The questionnaire consists of two forms that measure basic self-concept (form A) and ideal self-concept (form B). In both forms, there is 25 pair of contrasting personality traits, and the subject must evaluate herself/ himself according to those two traits and give herself/himself a score between 1 and 7. First, the scores obtained in forms A and B were subtracted, squared, added and then squared root to obtain the final score of an individual in the test. A total score of 0 to 7, 7.01 to 10 and 10.01 or higher indicate normal, moderate and weak self-concept, respectively. Aghajani (2008) reported the reliability coefficient of this questionnaire as 0.83 (14). Khadivi et al. (2011) verified the validity of the questionnaire by obtaining a correlation coefficient of 0.67 (15). In the present study, the reliability of the questionnaire was confirmed by obtaining a Cronbach's alpha coefficient of 0.80.
Snell (1995) first designed the sexual self-concept questionnaire for measuring individuals’ perception of sex (16). Ziaei (2013) validated the questionnaire in Iran. The Persian version of the questionnaire includes 78 items and 18 domains each of which consists of three to five items. The domains are classified into three dimensions: negative sexual self-concept, positive sexual self-concept and situational sexual self-concept. The minimum and maximum scores in the positive, negative and situational self-concept dimensions are 0-117, 0-64 and 0-77, respectively. The reliability of the questionnaire was found to be 0.76 to 0.89 (10). In the present study, the reliability of the positive, negative and situational self-concept dimensions was confirmed by obtaining Cronbach's alpha coefficient of 0.68, 0.85 and 0.73, respectively.
Data were expressed presented as mean ± standard deviation (SD). Normality of data was assessed using the Kolmogorov-Smirnov test. Data were analyzed accordingly using the Pearson's correlation coefficient and the Spearman's correlation test. SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA).
Mean age of participants was 28.88±5.14 years (range: 17-40 years). The majority of participants were married once (97.1%), homemaker (59%) and with bachelor's degrees (38.1%). In addition, most subjects were married for less than five years (Table 1).
Based on the results, 19% of the participants had normal general self-concept, 31.4% had moderate self-concept and 49.5% had weak self-concept. The mean scores of positive sexual self-concept, negative sexual self-concept and situational sexual self-concept were 118.9±24.85, 13.33±8.94 and 41.98± 10.53, respectively. Table 3 presents the mean score of the dimensions and subdomains of sexual self-concept.
There was no significant association between education level and self-concept scores in infertile women. The results of the Mann-Whitney test indicated a statistically significant difference in general self-concept and positive sexual self-concept scores between employed and homemaker infertile women. The results of the Kruskal-Wallis test indicated no statistically significant relationship between dimensions of sexual self-concept and the duration of the marriage or infertility.
The mean score of general self-concept, sexual self-concept and its dimensions in the levels of demographic variables such as level of education, duration of marriage, and duration of infertility were not statistically significant (P> 0.05).
There was a statistically significant difference between the mean score of general self-concept (P= 0.03) and positive sexual self-concept (P= 0.013) by occupation, but there was no statistically significant difference between the mean score of negative self-concept and position in occupation (p> 0.05).
Discussion
The present study examined the correlation between general self-concept and sexual self-concept of infertile women. We found no correlation between the general self-concept and sexual self-concept and its domains in infertile women. In a study by Mohammadi Nik et al. (2018), there were direct correlations between positive sexual self-concept and secure attachment and between negative sexual self-concept and insecure attachment (anxiety and avoidance) in married women of reproductive age. Moreover, women had high scores in the motivation subdomain to avoid high-risk sex (17). Similarly, we found that infertile women had the highest scores in the motivation subdomain to avoid high-risk sex. Salehi et al. (2015) reported that self-esteem and general self-concept had a significant positive correlation with sexual anxiety and fear of sex and a significant negative correlation with self-efficacy and sexual self-esteem (4). In another study, there was a positive correlation between self-esteem and sexual anxiety and a negative correlation between self-esteem and sexual self-efficacy in people with physical disabilities (18).
In our study, about half of the participants had lower self-concept. In line with this finding, Reisi et al. found that infertile women have lower self-concept compared with fertile women (19). Taghizadeh et al. (2015) found that candidates for receiving donor eggs had low self-concept and self-discrepancy (20).
In the positive sexual self-concept dimension, women had the highest scores in the motivation subdomain to avoid high-risk sexual behaviors and the lowest score in sexual optimism. In the negative sexual self-concept dimension, the subjects had the lowest scores (optimal status) in the sexual anxiety subdomain and the highest scores (sexual status) in the sexual monitoring subdomain. Saadat et al. (2014) found that all dimensions of sexual self-concept were weak in people with rheumatoid arthritis (21).
In the present study, there was a significant correlation between age and negative sexual self-concept so that the sexual self-concept score increased with age. In a study by Mohammadi Nik et al. (2014), age and duration of marriage had a strong correlation with sexual self-concept in women of reproductive age (17). It is necessary for sex therapists to take into account age as an important variable, especially in cases of infertility. In the present study, the general self-concept and positive sexual self-concept scores differed significantly between employed and homemaker women. In a previous cross-sectional study, it was found that women's education level had a positive correlation with positive and negative domains of sexual self-concept. In addition, women's occupation had a positive correlation with sexual self-esteem (22). According to the results, being employed and having higher education level could increase self-esteem, which ultimately strengthen positive sexual self-concept.
Conclusion
Our results indicate that there is no significant correlation between general self-concept and sexual self-concept in infertile women; hence, the general and sexual self-concepts of infertile women can be examined separately in evaluations and interventions. Given that age has a significant relationship with sexual self-concept, informing people to make early decisions for marriage and childbearing can help early diagnosis of infertility to increase the success of treatment. It is essential to develop programs aiming at improving self-concept and quality of life of infertile women. It is also recommended to study the association of general self-concept and sexual self-concept in infertile couples.
Acknowledgements
We are grateful to the staff of the Infertility Center of Gorgan and all participants as well as the Golestan University of Medical Sciences for their cooperation.
Funding source
This study was conducted with the financial support of Golestan University of Medical Sciences.
Ethical statement
This study was approved by the ethics committee of the Golestan University of Medical Sciences.
Conflict of interest
The authors declare that they have no conflict of interest.
The present study examined the correlation between general self-concept and sexual self-concept of infertile women. We found no correlation between the general self-concept and sexual self-concept and its domains in infertile women. In a study by Mohammadi Nik et al. (2018), there were direct correlations between positive sexual self-concept and secure attachment and between negative sexual self-concept and insecure attachment (anxiety and avoidance) in married women of reproductive age. Moreover, women had high scores in the motivation subdomain to avoid high-risk sex (17). Similarly, we found that infertile women had the highest scores in the motivation subdomain to avoid high-risk sex. Salehi et al. (2015) reported that self-esteem and general self-concept had a significant positive correlation with sexual anxiety and fear of sex and a significant negative correlation with self-efficacy and sexual self-esteem (4). In another study, there was a positive correlation between self-esteem and sexual anxiety and a negative correlation between self-esteem and sexual self-efficacy in people with physical disabilities (18).
In our study, about half of the participants had lower self-concept. In line with this finding, Reisi et al. found that infertile women have lower self-concept compared with fertile women (19). Taghizadeh et al. (2015) found that candidates for receiving donor eggs had low self-concept and self-discrepancy (20).
In the positive sexual self-concept dimension, women had the highest scores in the motivation subdomain to avoid high-risk sexual behaviors and the lowest score in sexual optimism. In the negative sexual self-concept dimension, the subjects had the lowest scores (optimal status) in the sexual anxiety subdomain and the highest scores (sexual status) in the sexual monitoring subdomain. Saadat et al. (2014) found that all dimensions of sexual self-concept were weak in people with rheumatoid arthritis (21).
In the present study, there was a significant correlation between age and negative sexual self-concept so that the sexual self-concept score increased with age. In a study by Mohammadi Nik et al. (2014), age and duration of marriage had a strong correlation with sexual self-concept in women of reproductive age (17). It is necessary for sex therapists to take into account age as an important variable, especially in cases of infertility. In the present study, the general self-concept and positive sexual self-concept scores differed significantly between employed and homemaker women. In a previous cross-sectional study, it was found that women's education level had a positive correlation with positive and negative domains of sexual self-concept. In addition, women's occupation had a positive correlation with sexual self-esteem (22). According to the results, being employed and having higher education level could increase self-esteem, which ultimately strengthen positive sexual self-concept.
Conclusion
Our results indicate that there is no significant correlation between general self-concept and sexual self-concept in infertile women; hence, the general and sexual self-concepts of infertile women can be examined separately in evaluations and interventions. Given that age has a significant relationship with sexual self-concept, informing people to make early decisions for marriage and childbearing can help early diagnosis of infertility to increase the success of treatment. It is essential to develop programs aiming at improving self-concept and quality of life of infertile women. It is also recommended to study the association of general self-concept and sexual self-concept in infertile couples.
Acknowledgements
We are grateful to the staff of the Infertility Center of Gorgan and all participants as well as the Golestan University of Medical Sciences for their cooperation.
Funding source
This study was conducted with the financial support of Golestan University of Medical Sciences.
Ethical statement
This study was approved by the ethics committee of the Golestan University of Medical Sciences.
Conflict of interest
The authors declare that they have no conflict of interest.
Author contributions
N G, T Z, E Kh and S Gh design the study, N G collecting the samples and data, M T doing statistical analysis, N G writing the manuscript, T Z, E Kh, M T and S GH editing the manuscript. All authors approved the final version of manuscript for submission.
Type of study: Original Article |
Subject:
Midwifery
References
1. Hilgard ER, Atkinson RC, Atkinson RL. Introduction to psychology. Oxford and IBH Publishing; 2009.
2. Liu LJ, Sun X, Zhang CL, Wang Y, Guo Q. A survey in rural China of parent-absence through migrant working: the impact on their children's self-concept and loneliness. BMC public health. 2010;10(1):1-8. [View at paplisher] [DOI] [PMID] [Google Scholar]
3. Afroz G, Ghasemzadeh S, Taziki T, Delgoshad. Effectiveness of mood regulation skills training on self-concept and social competence of students with learning disabilities. Journal of Learning Disabilities. 2014;3(3):6-24. [Persian] [View at paplisher] [Google Scholar]
4. Salehi M, Azarbayejani A, shafiei K, Ziaei T, Shayegh B. Self-esteem , general and sexual self-concepts in blind people. Journal of Research in Medical Sciences. 2015; 20(10). 930-6. [Persian] [View at paplisher] [DOI] [PMID] [Google Scholar]
5. O'Sullivan LF, Meyer-Bahlburg HFL, McKeague IW. The Development Of The Sexual Self-Concept Inventory For Early Adolescent Girls. Psychology of Women Quarterly. 2006;30(2):139-49. [View at paplisher] [DOI] [Google Scholar]
6. Hensel DJ, Fortenberry JD, O'Sullivan LF, Orr DP. The developmental association of sexual self-concept with sexual behavior among adolescent women. Journal of Adolescence. 2011;34(4):675-84. [View at paplisher] [DOI] [PMID] [Google Scholar]
7. Pai HC, Lee S. Sexual self-concept as influencing intended sexual health behaviour of young adolescent Taiwanese girls. J Clin Nurs. 2012;21(13-14):1988-97. [View at paplisher] [DOI] [PMID] [Google Scholar]
8. Rostosky SS, Dekhtyar O, Cupp PK, Anderman EM. Sexual self-concept and sexual self-efficacy in adolescents: a possible clue to promoting sexual health? J Sex Res. 2008;45(3):277-86. [View at paplisher] [DOI] [PMID] [Google Scholar]
9. Snell WE. The multidimensional sexual self-concept questionnaire. Handbook of sexuality-related measures. 1998:521-24. [Google Scholar]
10. Ziaei T, Khoei EM, Salehi M, Farajzadegan Z. Psychometric properties of the Farsi version of modified Multidimensional Sexual Self-concept Questionnaire. Iranian Journal of Nursing and Midwifery Research. 2013;18(6):439-45. [Persian] [Google Scholar]
11. Steinke EE, Wright DW, Chung ML, Moser DK. Sexual self-concept, anxiety, and self-efficacy predict sexual activity in heart failure and healthy elders. Heart Lung. 2008;37(5):323-33. [View at paplisher] [DOI] [PMID] [Google Scholar]
12. Tao P, Coates R, Maycock B. The impact of infertility on sexuality: A literature review. The Australasian medical journal. 2011;4(11):620-7. [DOI] [PMID] [Google Scholar]
13. Karaca A, Unsal G. Psychosocial Problems and Coping Strategies among Turkish Women with Infertility. Asian Nursing Research. 2015;9(3):243-50. [View at paplisher] [DOI] [PMID] [Google Scholar]
14. Aghajani S, Narimani M, Asiaei M. Emotional Intelligence and Self-concept in Ordinary and Gifted Students. JOEC. 2008; 8 (3) :317-323 [Persian] [View at paplisher] [Google Scholar]
15. Khadivi A, Vakili Mafakheri A. The relationship between acheivement motivation, locous of control, self-image and academic achievement in students of Tabriz. Journal of Educacational Sciences. 2011; 4(13):45-66. [Persian] [Google Scholar]
16. La Rocque CL, Cioe J. An evaluation of the relationship between body image and sexual avoidance. J Sex Res. 2011; 48(4):397-408. [View at paplisher] [DOI] [PMID] [Google Scholar]
17. Mohammadi Nik M, Modarres M, Ziaei T. The relation between sexual self-concepts and attachment styles in married women: A cross-sectional study. Nurs Pract Today. 2018;5(1):235-42. [Persian] [View at paplisher] [Google Scholar]
18. Salehi M, Kharaz Tavakol H, Shabani M, Ziaei T. The Relationship Between Self-Esteem and Sexual Self-Concept in People With Physical-Motor Disabilities. Iranian Red Crescent Medical Journal. 2015; 17(1):e25359. [Persian] [View at paplisher] [DOI] [Google Scholar]
19. Reisi M, Alidosti M, Asadi L. Self-Concept Among Infertile Women Receiving Oocyte Donation and Fertile Women. Researchsquare. 2020. [View at paplisher] [DOI] [Google Scholar]
20. Taghizadeh Z, Omani samani R, Kazemnejad A, Reisi M. Self-concept and self-discrepancy among the women receiving and donating oocyte. Hayat. 2015; 21 (3) :50-62. [Persian] [View at paplisher] [Google Scholar]
21. Saadat SH, Ramezani A, Ahmadi K. Sexual Self-Concept and General Health in Rheumatoid Arthritis Patients. Iran Red Crescent Med J. 2015; 17(10). [View at paplisher] [DOI] [Google Scholar]
22. Ziaei T, Farahmand Rad H, Rezaei Aval M, Roshandel G. The Relationship between Sexual Self-concept and Sexual Function in Women of Reproductive Age Referred to Health Centers in Gorgan, North East of Iran. JMRHE. 2017;5(3):969-77. [View at paplisher] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
