
Volume 20, Issue 1 (4-2023)
J Res Dev Nurs Midw 2023, 20(1): 61-65 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Modanloo M, Halakou S, Khoddam H, Nikpeyma N. Experience of health care providers in taking care of anxious patients under surgery with spinal anesthesia: A qualitative content analysis study. J Res Dev Nurs Midw 2023; 20 (1) :61-65
URL: http://nmj.goums.ac.ir/article-1-1435-en.html
URL: http://nmj.goums.ac.ir/article-1-1435-en.html



1- School of Nursing and Midwifery, Golestan University of Medical Sciences, Gorgan, Iran
2- School of Paramedical Sciences, Golestan University of Medical Sciences, Gorgan, Iran ,solmazhalakou@gmail.com
3- Nursing and midwifery faculty, Tehran University of Medical Sciences, Tehran, Iran
2- School of Paramedical Sciences, Golestan University of Medical Sciences, Gorgan, Iran ,
3- Nursing and midwifery faculty, Tehran University of Medical Sciences, Tehran, Iran
Full-Text [PDF 366 kb]
(1793 Downloads)
| Abstract (HTML) (3564 Views)
Full-Text: (1251 Views)
Introduction
Anxiety, the most common health problem and the second leading cause of disability worldwide (1, 2), is a common experience in patients before surgery (3, 4). It has been reported that 30% of hospitalized patients experience anxiety, even without surgery. However, this figure is 60% to 80% higher among patients who need surgery (5). According to Yuzkat (2020), approximately 75% of surgical candidates experience anxiety from the time they decide to undergo surgery until their discharge from the operating room (OR) (6).
Studies have reported that the cause of preoperative anxiety is related to disease severity, uncertainty around surgery, risk of anesthesia, lack of knowledge (6, 7), waiting for surgery (8), and fear of the unknown (9). Fear of regional anesthesia and its complications is also one of the most important sources of anxiety around surgery (10, 11). Spinal anesthesia is a type of regional anesthesia in which the anesthetic is injected into the cerebrospinal fluid in the intrathecal space. These patients are more anxious, as they are alert and receive surgical and OR stimuli in unknown environments (12, 13). Dias (2016) reported that almost one-third of patients who undergo surgery under regional anesthesia experience severe anxiety before surgery (14). Despite advancements in patient safety in both the surgery and anesthesia fields, these fears have not decreased over time (15). Patients who need surgery are still subject to anxiety and must be able to adapt in physical, psychological, and social dimensions (15).
Health care providers must be prepared to meet the challenges associated with anesthesia and surgery (16), which can be influenced by the patient's emotions (17). In this regard, the procedures performed by health care providers must be explored to involve responding to the needs of patients (17, 18). Qualitative research is a suitable method for gaining an in-depth description of people's views and experiences, which could contribute to the development of nursing science (18).
The aim of this study was to explore the experience of health care providers in taking care of anxious patients under surgery with spinal anesthesia.
Methods
This qualitative content analysis study was conducted at Shohada Hospital in Gonbad-e-Kavous city, northeastern Iran, from November 2020 to May 2021. This hospital is a referral center for patients who are candidates for gynecological surgery in the east of Golestan province.
Sixteen eligible health care providers (including nurse anesthetists, surgical technologists, nurses, and head nurses) who had experience in caring for anxious patients undergoing surgery with spinal anesthesia were selected for the study using purposive sampling. Inclusion criteria were willingness to participate in the study and having clinical work experience in taking care of these patients.
To collect data, semi-structured individual interviews were conducted in person at a pre-determined location by a member of the research team (S.H.). The duration of the interview was between 25 and 65 minutes. The purpose of the study was explained to the participants, and they signed written informed consent to conduct research. The participants were informed about the voluntary nature of their participation, the confidentiality of their information, and their right to withdraw from the study at any time. The individual interviews were conducted with a total of 16 health care providers, including 8 nurse anesthetists, 5 surgical technologists, 2 nurses, and 1 head nurse in the OR and surgical wards of the study setting. The researcher received assistance from the nurse manager of the hospital in coordinating the participation of the health care providers in the interviews.
The researcher first began the interview with a broad and open-ended question so that participants would narrate their overall experience (ie, “Please talk about your typical working day while caring for a patient who is a candidate for surgery”); then, the main questions were asked: “What is your experience in taking care of an anxious patient who is a candidate for spinal anesthesia?” To clarify ambiguities in answering previous questions, probing and reflective questions were used, such as "What do you mean?” The interviews were recorded and transcribed immediately after the end of the data collection. In addition to reporting the interview process and its key points, non-verbal messages from the participants (such as tone of voice, silence, and laughter) were also recorded as data for interpretation at the end of each interview.
Data were analyzed based on conventional content analysis in 3 phases: preparation, organization, and reporting. According to the analysis stages of qualitative data, interviews were read paragraph-by-paragraph, line-by-line, and word-by-word to gain a general understanding and for immersion in the data. Then, considering the aim of the study, meaning units and codes were extracted from interviews. Similar codes were grouped, and subcategories were made. By contrasting the subcategories, those that were related were merged to create main categories (19).
For the rigor and trustworthiness of data, the Lincoln and Guba approach was used (18). To ensure credibility, prolonged engagement with data was made, such that it took a long time to collect and analyze the data. The member check method was applied where after the transcription and coding process, the analyzed data were returned to 6 participants to ensure their accuracy. For dependability criteria, an external audit technique was used where 2 external nurses independently determined the codes and categories and compared their findings with each other. For the transferability of our findings, the researcher tried to fully describe the participants, sampling method, and time and setting of data collection. Furthermore, various participants were selected to explore their experiences. To ensure conformability, the researcher accurately recorded all stages of the research, allowing others to review the process and audit the data.
Results
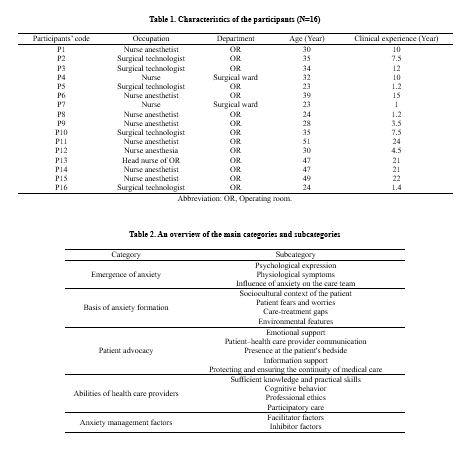
The mean age of participants was 33.81±9.63 years, with ages ranging from 23 to 51 years. Their clinical work experience ranged from 1 to 24 years (Table 1).
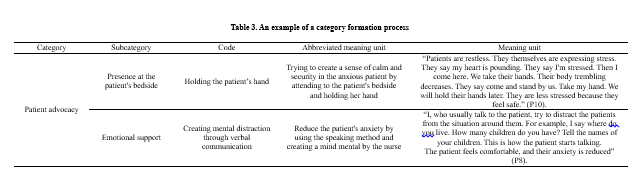
A total of 965 open codes were extracted from data analysis. There were 19 subcategories and 5 main categories (Table 2). Because of limitations in providing all open codes, a category formation process is presented in Table 3.
The main extracted categories were “emergence of anxiety,” “basis of anxiety formation,” “patient advocacy,” “abilities of health care providers,” and “anxiety management factors.
Emergence of anxiety
Anxiety can manifest in the form of physiological, emotional, and psychological features. “Patient physiological symptoms,” “patient emotional expression,” and “influence of anxiety on the care team” led to the formation of this category.
Physiological symptoms
Participants stated that anxiety affected patients’ physiological symptoms, such as blood pressure and heart rate.
“Patients who are anxious often have hypertension, while they have no history of this problem. They have tachycardia. They tremble with fear.” (P6).
Psychological expression
Participants indicated that the verbal expression of anxiety, collapsing fingers, crying, shivering, and restlessness are among the symptoms of patients’ preoperative anxiety.
“Patients are different in looking, speaking, and tone of voice. Some of them cry. They ask questions quickly without waiting for an answer. This indicates the patient's anxiety” (P14).
Influence of anxiety on the care team
Caring for clients who experience high levels of anxiety would stimulate the emotions of health care providers, thus having a direct impact on patient care outcomes.
“We had a patient who said that during her pregnancy, her husband had an accident and died. It affected our mood. We were upset” (P2).
Basis of the anxiety formation
Candidates for surgery become anxious in the OR due to the nature of the treatment and unknown issues. The subcategories of “patient fears and worries,” “sociocultural context of the patient,” “care-treatment gaps,” and “environmental features” have led to the formation of this category.
Patient fears and worries
Various factors (such as fear of strangers and foreigners and patient’s previous experiences) can cause anxiety. The most important fears of patients were anesthesia complications, such as observing the surgical scene, injection of anesthetic drugs into the spinal space, OR environment, and death prediction.
“The name of the OR is stressful. Even some patients, who have been operated on several times, are afraid because of the name of the OR. They say I may not regain consciousness. They are afraid of death” (P9).
Sociocultural context of the patient
Participants stated that the patient's personality background, low level of education, lack of surgery experience, family impact, and receiving incorrect information from the community about spinal anesthesia were among the causes of patients' anxiety.
“Patients have bad ideas about spinal anesthesia. They hear from family and friends that it has affected them negatively. We show them the spinal needle for these patients. At the end of surgery, I asked them how the anesthesia was. The patient said what I heard was very bad. But it was great!” (P11).
Care-treatment gaps
The participants emphasized the lack of certain necessary care or treatment, such as pre-anesthesia counseling, which led to patient anxiety.
“Our ideal approach is pre-anesthesia evaluation, not that the patient comes here to be diagnosed with a heart problem, maybe the patient will be identified after leaving the OR, and the patient should be calm in the hospital the night before. But it is not done in this hospital” (P13).
Environmental features
Participants indicated that the OR environment and the surgical ward did not have enough space to match the number of patients. This problem could increase patients’ anxiety.
“The ward space is small. Recovery room is not standard. The recovery space should be a separate and open space.” (P10).
Patient advocacy
Human health can be affected in various ways (such as emotional, psychological, social, emotional, and behavioral aspects), requiring comprehensive support to manage patient anxiety. This indicated that “psychological,” “patient–health care provider communication,” “presence at the patient's bedside,” “information support,” and “protect and ensure the continuity of medical care” led to creating the anxious patient advocacy category.
Emotional support
The health care providers tried to manage patients' anxiety via simple emotional supportive methods, such as distracting the patient, relaxation techniques, encouraging positive thinking, and deep reassuring breathing.
“I tell the patient who wants to go into the OR about its beauty and happiness; I tell them that there, our colleagues are present and they are very kind, and take care of you.” (P4).
Presence at the patient's bedside
This is an essential element of caring. Participants mentioned the presence of support, such as accompanying them when entering the OR and holding their hands.
“The patients insist on our presence. When I leave them to receive medicine or serum, the patients say, “Do not leave me!” I get stressed. Sometimes holding the patient’s hand during the spinal is effective to reduce their anxiety” (P8).
Patient–Health Care Provider Communication
Participants stated that verbal communication techniques, such as introducing themselves to the patient, appropriate tone of voice, kind speech, and appropriate non-verbal communication (such as smiling), have an effective role in managing patients' anxiety.
“We had a patient who was 14-15 years old. She was a uterine cyst surgery candidate. We told her that there was a possibility of a hysterectomy, then she canceled her operation and left. Later, her gynecologist said that the patient was operated in a private hospital, where they also told her that there was a possibility of hysterectomy, but their expression was different!” (P2).
Having a common language with the patient is one of the facilitators of effective communication, which is essential for providing quality nursing care based on a strong patient-caregiver relationship.
“Those whose language is different are much more stressed. I talk to the Turkmen language who is Turkmen (one of the Iranian tribes); these patients become very calm. I tell them that you are one of us. Then I explain to them that we are from a certain village.” (P1).
Information support
Participants stated that lack of patient information is one of the main causes of patients' anxiety. Using simple and understandable language with accurate use of terms is effective in reducing patient anxiety.
“One of the causes of anxiety is the fear of pain of anesthesia and surgery. So, we assure the patient and tell them an example that spinal anesthesia is like dental procedure, which you notice the movement of the doctor's hand, but do not feel pain” (P6).
Protecting and Ensuring the Continuity of Medical Care
In this study, the participants indicated that sedative drugs are used based on the severity of the patient's anxiety.
“Patients say that we are afraid to see many things around. We have to reassure them that we will use the curtain so that they do not see the surgery. However, they are still a little anxious that we, with the permission of the anesthetist, would give them midazolam to forget the procedure” (P1).
Abilities of health care providers
One of the tasks of health care providers is to reduce the anxiety of patients. “Sufficient knowledge and skills,” “participatory care,” “cognitive behavior,” and “professional ethics” led to the formation of this category.
Sufficient knowledge and practical skills
Participants stated that poor scientific and practical skills caused concerns among colleagues and the patient. Being an expert in care provision and treatment processes reduced patients' anxiety.
“The operation room staff must first relax and then have good scientific and practical skills. For example, yesterday’s incident! Anesthesiologists should first be calm. He excited condition by himself and shouted! The patient asks what is going to happen. The poor patient went to the point of the stroke. Her heart rate reached 147 beats, and this was due to the weakness in the science and practice of our anesthesiologist” (P12).
Participatory care
Excellent team working led to the creation of calming conditions for patients in the OR.
“We have to work together. We talk to the patient. The nurse anesthetist explains about anesthesia, and I talk about the surgery” (P5).
Cognitive behavior
This expressed that having patience, a willingness to listen, and maintaining calmness were among the effective cognitive characteristics of health care providers.
“I say to patients do not worry; I ask them about their children. I make them relax. Explaining what is going to happen is definitely effective” (P3).
Professional ethics
Participants mentioned that establishing and maintaining peace for patients who are candidates for surgery is possible through maintaining respect, privacy, and honesty with the patient.
“Some patients, as they do not have good clothing, do not feel comfortable” (P7).
Anxiety management
The subcategories of “facilitator factors” and “inhibitor factors” led to the formation of this category.
Facilitator factors
A good attitude of health care providers, such as trying to change the OR condition as context-based change, is one of the factors that facilitate the management of patient anxiety.
“We need to use context-based intervention by cooperating with each other based on cultural considerations. We intended to locate a television in the waiting room to provide them some information or to play music as ... We had no space ... " (P13).
Inhibitor factors
Participants stated that one of the barriers to implementing anxiety management was the lack of an incomplete patient care plan.
“How good it is for a patient who is a candidate for surgery to be hospitalized the day before it. We do not have the facilities. In our hospital, these things are seldom done. There are no facilities. How good would it be if we talked to the patient the night before surgery!” (P1).
Discussion
This study reported the experience of health care providers in taking care of anxious patients under surgery with spinal anesthesia. The main categories included “emergence of anxiety,” “basis of anxiety formation,” “patient advocacy,” “abilities of health care providers,” and “facilitators and inhibitors of patient anxiety management.”
Anxiety appears with physiological and psychological symptoms. This problem can affect the emotions and performance of health care providers. Several studies have reported that physiological problems occur in the body following anxiety (1, 7, 20). Arakelian (2018) reported that concerns of patients about anesthesia (including loss of body control, confinement of life in the hands of other people, and unknown words about surgery) could cause anxiety (21). Constantly receiving information from the OR environment and creating different questions in the minds of patients cause anxiety in patients. Factors such as observing people, surgical devices, and anesthesia in the OR environment affect patients' anxiety. Indeed, the reception of information from the OR environment and the generation of different questions in patients' minds cause concerns (22), which is consistent with the findings of the present study.
On the basis of the anxiety formation category, the sociocultural context of the patient was one of the mentioned dimensions. This was reported that cultural caring refers to a specific set of behaviors, attitudes, and skills that enable effective communication with people from different cultures (21). In this study, participants expressed that limited attention to cultural and social issues of surgical candidates led to increased anxiety in these patients. The health care providers should adapt the care to the client's culture by understanding the client's culture and accepting and respecting cultural differences (23).
Anxious patients who are candidates for surgery need the support of health care providers. Emotional support strategies are defined as protecting the patient’s privacy, listening to clients' fears, and creating a sense of control and relaxation in patients (24, 25). In this study, it was mentioned that verbal and non-verbal communication had a significant effect on the anxiety of patients who are candidates for surgery. One study found that health care providers should use a wide range of communication skills to provide information and instructions. By establishing a proper relationship with the patient, the symptoms of the patient's emotional stress could be checked, and the patient can be calmed down in time (25); this is consistent with the findings of our study. Informational support has been an important part of participants' statements. Lee (2018) reported that educational interventions reduce patients’ anxiety and enhance their satisfaction (26). Although written information is a good way to inform the patient of the unknown (27), in the present study, it was reported that written support for the patient had little effect on the patient's anxiety.
Based on the findings of our study, the knowledge and practice of the care team are directly related to patients' anxiety. Tamadoni (2020) emphasized the importance of clinical skills as essential competencies for nurses (28). It has been reported that anesthesiologists' assessments of patients' anxiety are often inaccurate, and they tend to underestimate their anxiety. Nurses also often misevaluate patients' anxiety (29). Health care providers must be able to predict the effects of ethical principles on their professional performance (30). Barari (2020) indicated that nurses had the closest relationship with patients compared to other members of the health care providers; thus, their behavior, especially in the surgical process, will have a greater impact on patients' anxiety (17). Vogelsang et al (2020 also noted that since nurses are often the first health care providers to meet patients upon admission to the OR, it is important to greet patients warmly and create a calm and friendly atmosphere (31), which is in line with the findings of our study.
According to the current study, if non-pharmacological supportive interventions are not effective in managing a patient's anxiety, health care providers may use pharmacological methods to ensure the continuity of medical care and protect the patient's well-being. Studies have reported that drugs can reduce patients' stress levels, though alternative interventions without the potential side effects of medication have also been introduced (26, 32).
Regarding the findings of this study, for patient anxiety management, context-based interventions, which are a combination of the health care providers, patient, and environment, should be conducted. According to studies, numerous interventions have been used to reduce patients' anxiety (33-35). Deeper information and context-based interventions are required to achieve better results (36).
One limitation of this study was the refusal of some health care providers to participate, which prevented us from using their experiences. However, we tried to mitigate this limitation by replacing them with other participants.
The participation of different members of health care providers related to the patients' surgery has been a positive point for exploring comprehensive experiences.
Conclusion
Health care providers consider that patient anxiety in spinal anesthesia is a common problem that can be affected by various factors. Therefore, to ensure patient comfort and cooperation during surgery, it is important to consider all necessary measures that create and maintain a comfortable environment for the patient. Different methods are used to manage patients' anxiety, but it is necessary to apply appropriate context-based interventions.
In terms of managerial applications, it is suggested that hospital managers should address patients' anxiety by taking into account the experiences of health care providers and identifying and solving the underlying issues. Increasing the productivity of health care providers can be facilitated by implementing educational courses as part of continuous training programs. According to the finding of this study, it is suggested to implement anxiety management interventions in hospital clinical departments and patient care clinics in future studies.
Acknowledgement
This study is a qualitative part of a larger nursing PhD thesis titled “Development, implementation, and evaluation of anxiety management program for women under gynecological surgery with spinal anesthesia: Action research study” (ethical code: IR.GOUMS.REC.1399.230). The authors would like to thank the Department of Research and Technology of Golestan University of Medical Sciences for funding the study, as well as the participants for their cooperation in this research project.
Funding sources
This study was done by financial support of Golestan University of Medical Sciences.
Ethical statement
The present study was approved by the center of the Ethics Committee of Golestan University of Medical Sciences, Iran (Code: IR.GOUMS.REC.1399.230).
Conflict of interest
The authors declare that there is no conflict of interest.
Author contributions
Mahnaz Modanloo: Principal investigator, who is the first supervisor of this doctoral dissertation, guided the study and contributed specifically to the analysis plan, Solmaz Halakou: Executor of the project who collected and analyzed quantitative data, drafted the paper, that was modified and supplemented by all other authors, Homeira Khoddam and Nasrin Nikpeyma: Consultants of project, helped to the interpretation of extracted data in all steps of study.
Anxiety, the most common health problem and the second leading cause of disability worldwide (1, 2), is a common experience in patients before surgery (3, 4). It has been reported that 30% of hospitalized patients experience anxiety, even without surgery. However, this figure is 60% to 80% higher among patients who need surgery (5). According to Yuzkat (2020), approximately 75% of surgical candidates experience anxiety from the time they decide to undergo surgery until their discharge from the operating room (OR) (6).
Studies have reported that the cause of preoperative anxiety is related to disease severity, uncertainty around surgery, risk of anesthesia, lack of knowledge (6, 7), waiting for surgery (8), and fear of the unknown (9). Fear of regional anesthesia and its complications is also one of the most important sources of anxiety around surgery (10, 11). Spinal anesthesia is a type of regional anesthesia in which the anesthetic is injected into the cerebrospinal fluid in the intrathecal space. These patients are more anxious, as they are alert and receive surgical and OR stimuli in unknown environments (12, 13). Dias (2016) reported that almost one-third of patients who undergo surgery under regional anesthesia experience severe anxiety before surgery (14). Despite advancements in patient safety in both the surgery and anesthesia fields, these fears have not decreased over time (15). Patients who need surgery are still subject to anxiety and must be able to adapt in physical, psychological, and social dimensions (15).
Health care providers must be prepared to meet the challenges associated with anesthesia and surgery (16), which can be influenced by the patient's emotions (17). In this regard, the procedures performed by health care providers must be explored to involve responding to the needs of patients (17, 18). Qualitative research is a suitable method for gaining an in-depth description of people's views and experiences, which could contribute to the development of nursing science (18).
The aim of this study was to explore the experience of health care providers in taking care of anxious patients under surgery with spinal anesthesia.
Methods
This qualitative content analysis study was conducted at Shohada Hospital in Gonbad-e-Kavous city, northeastern Iran, from November 2020 to May 2021. This hospital is a referral center for patients who are candidates for gynecological surgery in the east of Golestan province.
Sixteen eligible health care providers (including nurse anesthetists, surgical technologists, nurses, and head nurses) who had experience in caring for anxious patients undergoing surgery with spinal anesthesia were selected for the study using purposive sampling. Inclusion criteria were willingness to participate in the study and having clinical work experience in taking care of these patients.
To collect data, semi-structured individual interviews were conducted in person at a pre-determined location by a member of the research team (S.H.). The duration of the interview was between 25 and 65 minutes. The purpose of the study was explained to the participants, and they signed written informed consent to conduct research. The participants were informed about the voluntary nature of their participation, the confidentiality of their information, and their right to withdraw from the study at any time. The individual interviews were conducted with a total of 16 health care providers, including 8 nurse anesthetists, 5 surgical technologists, 2 nurses, and 1 head nurse in the OR and surgical wards of the study setting. The researcher received assistance from the nurse manager of the hospital in coordinating the participation of the health care providers in the interviews.
The researcher first began the interview with a broad and open-ended question so that participants would narrate their overall experience (ie, “Please talk about your typical working day while caring for a patient who is a candidate for surgery”); then, the main questions were asked: “What is your experience in taking care of an anxious patient who is a candidate for spinal anesthesia?” To clarify ambiguities in answering previous questions, probing and reflective questions were used, such as "What do you mean?” The interviews were recorded and transcribed immediately after the end of the data collection. In addition to reporting the interview process and its key points, non-verbal messages from the participants (such as tone of voice, silence, and laughter) were also recorded as data for interpretation at the end of each interview.
Data were analyzed based on conventional content analysis in 3 phases: preparation, organization, and reporting. According to the analysis stages of qualitative data, interviews were read paragraph-by-paragraph, line-by-line, and word-by-word to gain a general understanding and for immersion in the data. Then, considering the aim of the study, meaning units and codes were extracted from interviews. Similar codes were grouped, and subcategories were made. By contrasting the subcategories, those that were related were merged to create main categories (19).
For the rigor and trustworthiness of data, the Lincoln and Guba approach was used (18). To ensure credibility, prolonged engagement with data was made, such that it took a long time to collect and analyze the data. The member check method was applied where after the transcription and coding process, the analyzed data were returned to 6 participants to ensure their accuracy. For dependability criteria, an external audit technique was used where 2 external nurses independently determined the codes and categories and compared their findings with each other. For the transferability of our findings, the researcher tried to fully describe the participants, sampling method, and time and setting of data collection. Furthermore, various participants were selected to explore their experiences. To ensure conformability, the researcher accurately recorded all stages of the research, allowing others to review the process and audit the data.
Results
The mean age of participants was 33.81±9.63 years, with ages ranging from 23 to 51 years. Their clinical work experience ranged from 1 to 24 years (Table 1).
A total of 965 open codes were extracted from data analysis. There were 19 subcategories and 5 main categories (Table 2). Because of limitations in providing all open codes, a category formation process is presented in Table 3.
The main extracted categories were “emergence of anxiety,” “basis of anxiety formation,” “patient advocacy,” “abilities of health care providers,” and “anxiety management factors.
Emergence of anxiety
Anxiety can manifest in the form of physiological, emotional, and psychological features. “Patient physiological symptoms,” “patient emotional expression,” and “influence of anxiety on the care team” led to the formation of this category.
Physiological symptoms
Participants stated that anxiety affected patients’ physiological symptoms, such as blood pressure and heart rate.
“Patients who are anxious often have hypertension, while they have no history of this problem. They have tachycardia. They tremble with fear.” (P6).
Psychological expression
Participants indicated that the verbal expression of anxiety, collapsing fingers, crying, shivering, and restlessness are among the symptoms of patients’ preoperative anxiety.
“Patients are different in looking, speaking, and tone of voice. Some of them cry. They ask questions quickly without waiting for an answer. This indicates the patient's anxiety” (P14).
Influence of anxiety on the care team
Caring for clients who experience high levels of anxiety would stimulate the emotions of health care providers, thus having a direct impact on patient care outcomes.
“We had a patient who said that during her pregnancy, her husband had an accident and died. It affected our mood. We were upset” (P2).
Basis of the anxiety formation
Candidates for surgery become anxious in the OR due to the nature of the treatment and unknown issues. The subcategories of “patient fears and worries,” “sociocultural context of the patient,” “care-treatment gaps,” and “environmental features” have led to the formation of this category.
Patient fears and worries
Various factors (such as fear of strangers and foreigners and patient’s previous experiences) can cause anxiety. The most important fears of patients were anesthesia complications, such as observing the surgical scene, injection of anesthetic drugs into the spinal space, OR environment, and death prediction.
“The name of the OR is stressful. Even some patients, who have been operated on several times, are afraid because of the name of the OR. They say I may not regain consciousness. They are afraid of death” (P9).
Sociocultural context of the patient
Participants stated that the patient's personality background, low level of education, lack of surgery experience, family impact, and receiving incorrect information from the community about spinal anesthesia were among the causes of patients' anxiety.
“Patients have bad ideas about spinal anesthesia. They hear from family and friends that it has affected them negatively. We show them the spinal needle for these patients. At the end of surgery, I asked them how the anesthesia was. The patient said what I heard was very bad. But it was great!” (P11).
Care-treatment gaps
The participants emphasized the lack of certain necessary care or treatment, such as pre-anesthesia counseling, which led to patient anxiety.
“Our ideal approach is pre-anesthesia evaluation, not that the patient comes here to be diagnosed with a heart problem, maybe the patient will be identified after leaving the OR, and the patient should be calm in the hospital the night before. But it is not done in this hospital” (P13).
Environmental features
Participants indicated that the OR environment and the surgical ward did not have enough space to match the number of patients. This problem could increase patients’ anxiety.
“The ward space is small. Recovery room is not standard. The recovery space should be a separate and open space.” (P10).
Patient advocacy
Human health can be affected in various ways (such as emotional, psychological, social, emotional, and behavioral aspects), requiring comprehensive support to manage patient anxiety. This indicated that “psychological,” “patient–health care provider communication,” “presence at the patient's bedside,” “information support,” and “protect and ensure the continuity of medical care” led to creating the anxious patient advocacy category.
Emotional support
The health care providers tried to manage patients' anxiety via simple emotional supportive methods, such as distracting the patient, relaxation techniques, encouraging positive thinking, and deep reassuring breathing.
“I tell the patient who wants to go into the OR about its beauty and happiness; I tell them that there, our colleagues are present and they are very kind, and take care of you.” (P4).
Presence at the patient's bedside
This is an essential element of caring. Participants mentioned the presence of support, such as accompanying them when entering the OR and holding their hands.
“The patients insist on our presence. When I leave them to receive medicine or serum, the patients say, “Do not leave me!” I get stressed. Sometimes holding the patient’s hand during the spinal is effective to reduce their anxiety” (P8).
Patient–Health Care Provider Communication
Participants stated that verbal communication techniques, such as introducing themselves to the patient, appropriate tone of voice, kind speech, and appropriate non-verbal communication (such as smiling), have an effective role in managing patients' anxiety.
“We had a patient who was 14-15 years old. She was a uterine cyst surgery candidate. We told her that there was a possibility of a hysterectomy, then she canceled her operation and left. Later, her gynecologist said that the patient was operated in a private hospital, where they also told her that there was a possibility of hysterectomy, but their expression was different!” (P2).
Having a common language with the patient is one of the facilitators of effective communication, which is essential for providing quality nursing care based on a strong patient-caregiver relationship.
“Those whose language is different are much more stressed. I talk to the Turkmen language who is Turkmen (one of the Iranian tribes); these patients become very calm. I tell them that you are one of us. Then I explain to them that we are from a certain village.” (P1).
Information support
Participants stated that lack of patient information is one of the main causes of patients' anxiety. Using simple and understandable language with accurate use of terms is effective in reducing patient anxiety.
“One of the causes of anxiety is the fear of pain of anesthesia and surgery. So, we assure the patient and tell them an example that spinal anesthesia is like dental procedure, which you notice the movement of the doctor's hand, but do not feel pain” (P6).
Protecting and Ensuring the Continuity of Medical Care
In this study, the participants indicated that sedative drugs are used based on the severity of the patient's anxiety.
“Patients say that we are afraid to see many things around. We have to reassure them that we will use the curtain so that they do not see the surgery. However, they are still a little anxious that we, with the permission of the anesthetist, would give them midazolam to forget the procedure” (P1).
Abilities of health care providers
One of the tasks of health care providers is to reduce the anxiety of patients. “Sufficient knowledge and skills,” “participatory care,” “cognitive behavior,” and “professional ethics” led to the formation of this category.
Sufficient knowledge and practical skills
Participants stated that poor scientific and practical skills caused concerns among colleagues and the patient. Being an expert in care provision and treatment processes reduced patients' anxiety.
“The operation room staff must first relax and then have good scientific and practical skills. For example, yesterday’s incident! Anesthesiologists should first be calm. He excited condition by himself and shouted! The patient asks what is going to happen. The poor patient went to the point of the stroke. Her heart rate reached 147 beats, and this was due to the weakness in the science and practice of our anesthesiologist” (P12).
Participatory care
Excellent team working led to the creation of calming conditions for patients in the OR.
“We have to work together. We talk to the patient. The nurse anesthetist explains about anesthesia, and I talk about the surgery” (P5).
Cognitive behavior
This expressed that having patience, a willingness to listen, and maintaining calmness were among the effective cognitive characteristics of health care providers.
“I say to patients do not worry; I ask them about their children. I make them relax. Explaining what is going to happen is definitely effective” (P3).
Professional ethics
Participants mentioned that establishing and maintaining peace for patients who are candidates for surgery is possible through maintaining respect, privacy, and honesty with the patient.
“Some patients, as they do not have good clothing, do not feel comfortable” (P7).
Anxiety management
The subcategories of “facilitator factors” and “inhibitor factors” led to the formation of this category.
Facilitator factors
A good attitude of health care providers, such as trying to change the OR condition as context-based change, is one of the factors that facilitate the management of patient anxiety.
“We need to use context-based intervention by cooperating with each other based on cultural considerations. We intended to locate a television in the waiting room to provide them some information or to play music as ... We had no space ... " (P13).
Inhibitor factors
Participants stated that one of the barriers to implementing anxiety management was the lack of an incomplete patient care plan.
“How good it is for a patient who is a candidate for surgery to be hospitalized the day before it. We do not have the facilities. In our hospital, these things are seldom done. There are no facilities. How good would it be if we talked to the patient the night before surgery!” (P1).
Discussion
This study reported the experience of health care providers in taking care of anxious patients under surgery with spinal anesthesia. The main categories included “emergence of anxiety,” “basis of anxiety formation,” “patient advocacy,” “abilities of health care providers,” and “facilitators and inhibitors of patient anxiety management.”
Anxiety appears with physiological and psychological symptoms. This problem can affect the emotions and performance of health care providers. Several studies have reported that physiological problems occur in the body following anxiety (1, 7, 20). Arakelian (2018) reported that concerns of patients about anesthesia (including loss of body control, confinement of life in the hands of other people, and unknown words about surgery) could cause anxiety (21). Constantly receiving information from the OR environment and creating different questions in the minds of patients cause anxiety in patients. Factors such as observing people, surgical devices, and anesthesia in the OR environment affect patients' anxiety. Indeed, the reception of information from the OR environment and the generation of different questions in patients' minds cause concerns (22), which is consistent with the findings of the present study.
On the basis of the anxiety formation category, the sociocultural context of the patient was one of the mentioned dimensions. This was reported that cultural caring refers to a specific set of behaviors, attitudes, and skills that enable effective communication with people from different cultures (21). In this study, participants expressed that limited attention to cultural and social issues of surgical candidates led to increased anxiety in these patients. The health care providers should adapt the care to the client's culture by understanding the client's culture and accepting and respecting cultural differences (23).
Anxious patients who are candidates for surgery need the support of health care providers. Emotional support strategies are defined as protecting the patient’s privacy, listening to clients' fears, and creating a sense of control and relaxation in patients (24, 25). In this study, it was mentioned that verbal and non-verbal communication had a significant effect on the anxiety of patients who are candidates for surgery. One study found that health care providers should use a wide range of communication skills to provide information and instructions. By establishing a proper relationship with the patient, the symptoms of the patient's emotional stress could be checked, and the patient can be calmed down in time (25); this is consistent with the findings of our study. Informational support has been an important part of participants' statements. Lee (2018) reported that educational interventions reduce patients’ anxiety and enhance their satisfaction (26). Although written information is a good way to inform the patient of the unknown (27), in the present study, it was reported that written support for the patient had little effect on the patient's anxiety.
Based on the findings of our study, the knowledge and practice of the care team are directly related to patients' anxiety. Tamadoni (2020) emphasized the importance of clinical skills as essential competencies for nurses (28). It has been reported that anesthesiologists' assessments of patients' anxiety are often inaccurate, and they tend to underestimate their anxiety. Nurses also often misevaluate patients' anxiety (29). Health care providers must be able to predict the effects of ethical principles on their professional performance (30). Barari (2020) indicated that nurses had the closest relationship with patients compared to other members of the health care providers; thus, their behavior, especially in the surgical process, will have a greater impact on patients' anxiety (17). Vogelsang et al (2020 also noted that since nurses are often the first health care providers to meet patients upon admission to the OR, it is important to greet patients warmly and create a calm and friendly atmosphere (31), which is in line with the findings of our study.
According to the current study, if non-pharmacological supportive interventions are not effective in managing a patient's anxiety, health care providers may use pharmacological methods to ensure the continuity of medical care and protect the patient's well-being. Studies have reported that drugs can reduce patients' stress levels, though alternative interventions without the potential side effects of medication have also been introduced (26, 32).
Regarding the findings of this study, for patient anxiety management, context-based interventions, which are a combination of the health care providers, patient, and environment, should be conducted. According to studies, numerous interventions have been used to reduce patients' anxiety (33-35). Deeper information and context-based interventions are required to achieve better results (36).
One limitation of this study was the refusal of some health care providers to participate, which prevented us from using their experiences. However, we tried to mitigate this limitation by replacing them with other participants.
The participation of different members of health care providers related to the patients' surgery has been a positive point for exploring comprehensive experiences.
Conclusion
Health care providers consider that patient anxiety in spinal anesthesia is a common problem that can be affected by various factors. Therefore, to ensure patient comfort and cooperation during surgery, it is important to consider all necessary measures that create and maintain a comfortable environment for the patient. Different methods are used to manage patients' anxiety, but it is necessary to apply appropriate context-based interventions.
In terms of managerial applications, it is suggested that hospital managers should address patients' anxiety by taking into account the experiences of health care providers and identifying and solving the underlying issues. Increasing the productivity of health care providers can be facilitated by implementing educational courses as part of continuous training programs. According to the finding of this study, it is suggested to implement anxiety management interventions in hospital clinical departments and patient care clinics in future studies.
Acknowledgement
This study is a qualitative part of a larger nursing PhD thesis titled “Development, implementation, and evaluation of anxiety management program for women under gynecological surgery with spinal anesthesia: Action research study” (ethical code: IR.GOUMS.REC.1399.230). The authors would like to thank the Department of Research and Technology of Golestan University of Medical Sciences for funding the study, as well as the participants for their cooperation in this research project.
Funding sources
This study was done by financial support of Golestan University of Medical Sciences.
Ethical statement
The present study was approved by the center of the Ethics Committee of Golestan University of Medical Sciences, Iran (Code: IR.GOUMS.REC.1399.230).
Conflict of interest
The authors declare that there is no conflict of interest.
Author contributions
Mahnaz Modanloo: Principal investigator, who is the first supervisor of this doctoral dissertation, guided the study and contributed specifically to the analysis plan, Solmaz Halakou: Executor of the project who collected and analyzed quantitative data, drafted the paper, that was modified and supplemented by all other authors, Homeira Khoddam and Nasrin Nikpeyma: Consultants of project, helped to the interpretation of extracted data in all steps of study.
Type of study: Original Article |
Subject:
Nursing
References
1. Abadi F, Abedi F, Fereidouni Z, Amirkhani M, Karimi S, Kalyani M.N. Effect of acupressure on preoperative cesarean section anxiety. Journal of Acupuncture and Meridian Studies. 2018;11(6):361-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Kasturi S, Oguoma VM, Grant JB, Niyonsenga T, Mohanty I. Prevalence rates of depression and anxiety among young rural and urban Australians: a systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2023;20(1):800. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Cakmak M, Kose I, Zinzircioglu C, Karaman Y, Tekgul ZT, Pektas S, et al. Effect of video-based education on anxiety and satisfaction of patients undergoing spinal anesthesia. Revista brasileira de anestesiologia. 2018;68(3):274-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Dagli R, Avcu M, Metin M, Kiymaz S, Ciftci H. The effects of aromatherapy using rose oil (Rosa damascena Mill.) on preoperative anxiety: A prospective randomized clinical trial. European Journal of Integrative Medicine. 2019;26:37-42. [View at Publisher] [DOI] [Google Scholar]
5. Nasiri E, Birami M, Mahdavinoor SMM, Rafiei MH. Health care team understanding of patients' desire for information on surgery and anesthesia: A cross-sectional study. Perioperative Care and Operating Room Management. 2020;21:100134. [View at Publisher] [DOI] [Google Scholar]
6. Yuzkat N, Soyalp C, Turk O, Keskin S, Gulhas N. Effects of showing the operating room on preoperative anxiety and hemodynamics among patients with hypertension: A randomized controlled trial. Clinical and Experimental Hypertension. 2020;42(6):553-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Jung K-H, Park J-H, Ahn J-W, Park K-B. Surgery-related anxiety on geriatric patients undergoing total knee arthroplasty: a retrospective observational study. BMC Musculoskeletal Disorders. 2023;24(1):161e1-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Ghanizadeh L, Hosseini S-R, Zaker MR. Preoperative Anxiety and Related Factors in Patients Undergoing Elective Surgery. Zanko Journal of Medical Sciences. 2020;21(70):1-12. [View at Publisher] [Google Scholar]
9. Wen-Ping L, Pao-Yuan W, Meng-Ying L, Lun-Hui H, Whei-Mei S. Music listening alleviates anxiety and physiological responses in patients receiving spinal anesthesia. Complementary Therapies in Medicine. 2017;31:8-13. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Yılmaz İnal F, Yılmaz Y, Daşkaya H, Toptaş M, Koçoğlu H, Uysal H, et al. Evaluation of the attitudes of surgeons about regional anesthesia: a survey study. Local and Regional Anesthesia. 2019:89-95. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Gürler H, Yılmaz M, Türk KE. Preoperative anxiety levels in surgical patients: A comparison of three different scale scores. Journal of PeriAnesthesia Nursing. 2022;37(1):69-74. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Pulkkinen M, Junttila K, Lindwall L. The perioperative dialogue-a model of caring for the patient undergoing a hip or a knee replacement surgery under spinal anaesthesia. Scandinavian Journal of Caring Sciences. 2016;30(1):145-53. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Ikyul B, Man LH, Myung-Haeng H, MyeongSoo L. Intra-operative music listening for anxiety, the BIS index, and the vital signs of patients undergoing regional anesthesia. Complementary Therapies in Medicine. 2014;22(2):251-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Dias R, Baliarsing L, Barnwal N, Mogal S, Gujjar P. Role of pre-operative multimedia video information in allaying anxiety related to spinal anaesthesia: A randomised controlled trial. Indian Journal of Anesthesia. 2016;60(11):843-47. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Rastgarian A, Esmaelpour N, Javadpour S, Sadeghi S, Kalani N, Sepidkar A, et al. preoperative anxiety in hospitalzed patients: A descriptive cross-sectional study. Medical Journal of Mashhad University of Medical Sciences. 2020;63(1):2118-209. [View at Publisher] [DOI] [Google Scholar]
16. Pestana-Santos M, Pestana-Santos A, Cabral IE, Santos MR, Lomba L. Nurses' Views on How to Best Design a Program to Prevent Adolescents' Anxiety in the Perioperative Period. A Qualitative Study. Journal of PeriAnesthesia Nursing. 2022;37(4):458-66. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Barari F, Mollahadi M, Moshtagh Z, Salaree M. Investigating the Effect of Rhythmic Breathing Training by Teach Back Method on Anxiety in Patients Undergoing Tympanoplasty. Education Strategies in Medical Sciences. 2020;9(3):172.8. [View at Publisher] [Google Scholar]
18. Polit DF, Beck CT. Essentials of nursing research: Appraising evidence for nursing practice: Lippincott Williams & Wilkins; 2017. [Google Scholar]
19. Elo S, Kyngäs H. The qualitative content analysis process. Journal of advanced nursing. 2008;62(1):107-15. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Ju X, Feng J, Yang J, Ge L, Liu X. Factors influencing the preoperative anxiety in lung cancer patients undergoing video-assisted thoracoscopic surgery: The role of information needs, illness perception and patient trust. Journal of Psychosomatic Research. 2023:e111374. [View at Publisher] [DOI] [PMID] [Google scholar]
21. Arakelian E, Laurssen E, Oster C. Older Patients' Worries in Connection With General Anesthesia and Surgery-A Qualitative Study. Journal of PeriAnesthesia Nursing. 2018;33(6):822-33. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Haugen AS, Eide GE, Olsen MV, Haukeland B, Remme AR, Wahl AK. Anxiety in the operating theatre: a study of frequency and environmental impact in patients having local, plexus or regional anaesthesia. Journal of Clinical Nursing. 2009;18(16):2301-10. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Karatay G, Bowers B, Karadağ E, Demir M. Cultural perceptions and clinical experiences of nursing students in Eastern Turkey. International Nursing Review. 2016;63(4):547-54. [View at Publisher] [DOI] [PMID] [Google Scholar]
24. Weisfeld CC, Turner JA, Bowen JI, Eissa R, Roelk B, Ko A, et al. Dealing with anxious patients: an integrative review of the literature on nonpharmaceutical interventions to reduce anxiety in patients undergoing medical or dental procedures. The Journal of Alternative and Complementary Medicine. 2021;27(9):727-37.
https://doi.org/10.1089/acm.2020.0504 [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Babaii A, Mohammadi E, Sadooghiasl A. The meaning of the empathetic nurse-patient communication: A qualitative study. Journal of Patient Experience. 2021;8(1):e1-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Lee C, Liu J, Lin S, TY Hsu, Lin C, Lin L. Effects of Educational Intervention on State Anxiety and Pain in People Undergoing Spinal Surgery: A Randomized Controlled Trial. Pain Management Nursing. 2018;19(2):163-71. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Pokharel K, Bhattarai B, Tripathi M, Khatiwada S, Subedi A. Nepalese patients' anxiety and concerns before surgery. Journal of Clinical Anesthesia. 2011;23(5):372-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Vand Tamadoni B, Shahbazi S, Seyedrasooli A, Gilani N, Gholizadeh L. A survey of clinical competence of new nurses working in emergency department in Iran: A descriptive, cross‐sectional study. Nursing Open. 2020;7(6):1896-901. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Jlala HA, Bedforth NM, Hardman JG. Anesthesiologists' perception of patients' anxiety under regional anesthesia. Local and Regional anesthesia. 2010;3:65. [View at Publisher] [DOI] [PMID] [Google Scholar]
30. Doherty RF, Purtilo RB. Ethical Dimensions in the Health Professions-E-Book: Elsevier Health Sciences; 2015. [Google Scholar]
31. von Vogelsang AC, Swenne CL, Gustafsson BÅ, Falk Brynhildsen K. Operating theatre nurse specialist competence to ensure patient safety in the operating theatre: A discursive paper. Nursing open. 2020;7(2):495-502. [View at Publisher] [DOI] [PMID] [Google Scholar]
32. Ilkkaya N, Ustun F, Sener E, Kaya C, Ustun Y, E Koksal, et al. The effects of music, white noise, and ambient noise on sedation and anxiety in patients under spinal anesthesia during surgery Journal of PeriAnesthesia Nursing. 2014;29(5):418-26. [View at Publisher] [DOI] [PMID] [Google Scholar]
33. Jaruzel CB, Gregoski M, Mueller M, Faircloth A, Kelechi T. Aromatherapy for preoperative anxiety: A pilot study. Journal of Perianesthesia Nursing. 2019;34(2):259-64. [View at Publisher] [DOI] [PMID] [Google Scholar]
34. Heshmatifar N, Mohebbi M, Borzoee F, Rakhhani M. The Effect of Mental Imagery on Preoperative Anxiety of Elective Hernia. Complementary Medicine Journal. 2020;9(4):3930-9. [View at Publisher] [DOI] [Google Scholar]
35. Ortiz J, Wang S, Elayda MA, Tolpin DA. [Preoperative patient education: can we improve satisfaction and reduce anxiety?]. Brazilian Journal of Anesthesiology. 2015;65(1):7-13. [View at Publisher] [DOI] [PMID] [Google Scholar]
36. Halakou S, Khoddam H, Nikpeyma N, Modanloo M. Development and implementation of anxiety management program for women under gynecological surgery with spinal anesthesia: Protocol of action research study. Journal of Education and Health Promotion. 2022;11(1):374. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
