
Volume 20, Issue 2 (10-2023)
J Res Dev Nurs Midw 2023, 20(2): 44-49 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Miri K, mohamadi E, Vanaki Z, Mazloum S R. The life cycle of nursing organizations and role development in Iran: A situational analysis. J Res Dev Nurs Midw 2023; 20 (2) :44-49
URL: http://nmj.goums.ac.ir/article-1-1472-en.html
URL: http://nmj.goums.ac.ir/article-1-1472-en.html



1- Department of Nursing, School of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran , mirikheizaran@yahoo.ie
2- Department of Nursing, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
3- Department of Medical, Surgical Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
2- Department of Nursing, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
3- Department of Medical, Surgical Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
Full-Text [PDF 749 kb]
(1146 Downloads)
| Abstract (HTML) (2673 Views)
Full-Text: (562 Views)
Introduction
Nursing organizations play a critical role in advancing the nursing profession. These organizations establish positions on key nursing issues and work to generate and promote nursing roles in various fields (1). Their growth is followed by the development of the functions of nursing (2). Nursing organizations have a crucial role in improving the role of nursing (1), which is related to the corporate life cycle.
The life cycle of nursing organizations and role development in nursing is a complex and dynamic process, influenced by various factors such as managed care, professional, managerial, and policy forces, and the evolving healthcare system. These models suggest that, much like a biological organism, an organization goes through various stages of development, from inception to growth, maturity, and eventual decline or renewal, each with its own set of challenges and organizational needs. Gardner’s 1965 contribution laid the foundation for understanding how organizations evolve and adapt over time.
Indeed, like people and plants, organizations “have a green and supple youth, a time of flourishing strength, and a gnarled old age” (3). A central tenet of life cycle theory is that organizations move through a series of phases. Hanks et al (1993) defined a life cycle phase as a unique configuration of variables related to organizational context or structure (4). Therefore, OLC includes a sequence of events that describe how things change over time.
The management and leadership used in nursing professional organizations, their interaction, and their quantitative and qualitative changes in the evolutionary cycle directly affect the development of the nursing role (5). In the past, nurses have been routinely treated as physician assistants (6), and there has been no professional nursing organization. The advancement of medical sciences, changing societal needs, and the creation of professional organizations made the role of nurses more complex and variable (5). Therefore, the nursing role shifted from general to specialized (7). Managers are constantly seeking to understand how they can make changes at different levels, both within the health system and professional nursing organizations in each country. It is obvious that such a perception can led to changes in nurses' roles and affect the safety and quality of care. The mission and role of these organizations vary in different countries.
Regulatory bodies in the US operate separately from professional systems and trade :union:s (8). Over the last 30 years, more than 65 professional nursing associations and organizations have been established at the state level. In the last hundred years, 5 large nursing associations have been established at the national and international levels (2). These conditions do not exist in some countries. For example, the regulatory bodies are all the same in some provinces of Canada and Portugal. In some jurisdictions, the functions of regulatory bodies, professional associations, and trade :union:s coexist. For example, in some Canadian provinces and Spain, the roles of regulators and professional associations are held by the same organization (9). However, in Iran, nursing professional associations play a key role in helping regulators develop nursing policies and laws.
Recent quantitative and qualitative studies conducted in Iran over the last decade have reported that the development of the nursing role in the country is ambiguous and undesirable (7, 10,11). Also, only 1 nursing organization has been examined in these studies. Therefore, these studies have shown the slow development of the nursing role in Iran. However, no study has analyzed the situation of professional nursing organizations and their effects on Iran's nursing role development. In reality, what roles do these professional organizations play in establishing and developing the nursing profession? What patterns have arisen in the situation study approach? How do they rise, and do their circumstances impact the development of the role of nurses? Really, what's their life cycle, and how do they support the nursing profession? Therefore, this research was undertaken to examine the condition of nursing organizations, their life cycles, their experiences, and their effect on the development of nursing roles.
Methods
Context and setting
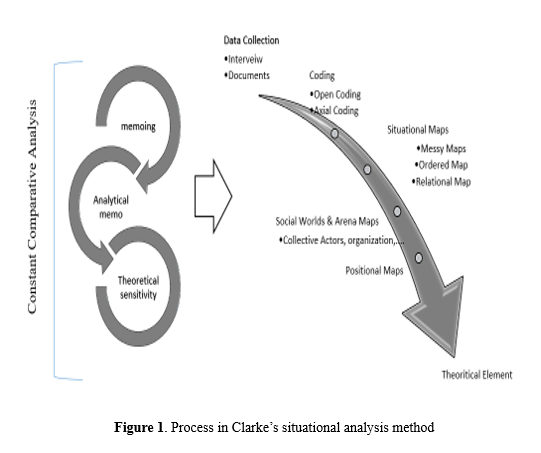
The Clark situational analysis (Figure 1) was used as a qualitative analysis approach based on discourses beyond pragmatism to describe the complexities of social processes (12). Given the complexities of professional roles in the health care system, which are influenced by cultural, economic, and social variables, the Clark situational analysis method can be useful. The situational analysis, which involves situational mapping and preparation of social and positional maps, is introduced as a desirable method for this study. Clark has described the situation mapping process in several steps and includes the following steps:
Nursing organizations play a critical role in advancing the nursing profession. These organizations establish positions on key nursing issues and work to generate and promote nursing roles in various fields (1). Their growth is followed by the development of the functions of nursing (2). Nursing organizations have a crucial role in improving the role of nursing (1), which is related to the corporate life cycle.
The life cycle of nursing organizations and role development in nursing is a complex and dynamic process, influenced by various factors such as managed care, professional, managerial, and policy forces, and the evolving healthcare system. These models suggest that, much like a biological organism, an organization goes through various stages of development, from inception to growth, maturity, and eventual decline or renewal, each with its own set of challenges and organizational needs. Gardner’s 1965 contribution laid the foundation for understanding how organizations evolve and adapt over time.
Indeed, like people and plants, organizations “have a green and supple youth, a time of flourishing strength, and a gnarled old age” (3). A central tenet of life cycle theory is that organizations move through a series of phases. Hanks et al (1993) defined a life cycle phase as a unique configuration of variables related to organizational context or structure (4). Therefore, OLC includes a sequence of events that describe how things change over time.
The management and leadership used in nursing professional organizations, their interaction, and their quantitative and qualitative changes in the evolutionary cycle directly affect the development of the nursing role (5). In the past, nurses have been routinely treated as physician assistants (6), and there has been no professional nursing organization. The advancement of medical sciences, changing societal needs, and the creation of professional organizations made the role of nurses more complex and variable (5). Therefore, the nursing role shifted from general to specialized (7). Managers are constantly seeking to understand how they can make changes at different levels, both within the health system and professional nursing organizations in each country. It is obvious that such a perception can led to changes in nurses' roles and affect the safety and quality of care. The mission and role of these organizations vary in different countries.
Regulatory bodies in the US operate separately from professional systems and trade :union:s (8). Over the last 30 years, more than 65 professional nursing associations and organizations have been established at the state level. In the last hundred years, 5 large nursing associations have been established at the national and international levels (2). These conditions do not exist in some countries. For example, the regulatory bodies are all the same in some provinces of Canada and Portugal. In some jurisdictions, the functions of regulatory bodies, professional associations, and trade :union:s coexist. For example, in some Canadian provinces and Spain, the roles of regulators and professional associations are held by the same organization (9). However, in Iran, nursing professional associations play a key role in helping regulators develop nursing policies and laws.
Recent quantitative and qualitative studies conducted in Iran over the last decade have reported that the development of the nursing role in the country is ambiguous and undesirable (7, 10,11). Also, only 1 nursing organization has been examined in these studies. Therefore, these studies have shown the slow development of the nursing role in Iran. However, no study has analyzed the situation of professional nursing organizations and their effects on Iran's nursing role development. In reality, what roles do these professional organizations play in establishing and developing the nursing profession? What patterns have arisen in the situation study approach? How do they rise, and do their circumstances impact the development of the role of nurses? Really, what's their life cycle, and how do they support the nursing profession? Therefore, this research was undertaken to examine the condition of nursing organizations, their life cycles, their experiences, and their effect on the development of nursing roles.
Methods
Context and setting
The Clark situational analysis (Figure 1) was used as a qualitative analysis approach based on discourses beyond pragmatism to describe the complexities of social processes (12). Given the complexities of professional roles in the health care system, which are influenced by cultural, economic, and social variables, the Clark situational analysis method can be useful. The situational analysis, which involves situational mapping and preparation of social and positional maps, is introduced as a desirable method for this study. Clark has described the situation mapping process in several steps and includes the following steps:
- Data collection stage: interviews, documentation, etc.
- Coding: open coding and axial coding of data.
- Situational maps: The purpose of conducting a situational map is to provide a comprehensive description of all the relevant human and non-human components of a research situation, with the aim of facilitating a clear understanding of the situation.
- Maps of arenas and social worlds: In this map, the actions of people both as individuals and as members of social worlds in ongoing discourses are examined.
Positional Map: This map shows a deep understanding of the data in the main adopted and unadopted states.
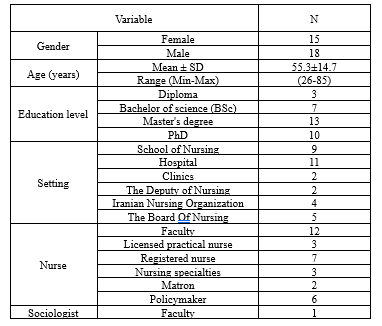
The research community of this study included registered nurses (RNs) and licensed practical nurses (LPNs) in health care centers and clinics, instructors of nursing schools, and nurse managers. Some repeated patterns emerged after 17 interviews, and data saturation was achieved after 24 interviews. However, we conducted 33 interviews to ensure the sufficiency of data. Data were collected through in-depth semi-structured interviews with 33 Iranian nurses. The location of the interviews was different based on the interests of the participants (at work, hospital, home, etc.) (Table 1). The sources of data collection include interviews, analysis of documents at Dr Madah Association and the National Library of Iran, statistics, government documents, international reports, and historical articles about nursing organizations, as well as reports on the role of LPNs and RNs. Participants were selected using purposive sampling from September 2018 to February 2021. Written consent was obtained from the participants. The interviews, conducted by the first author, lasted 30 to 60 minutes per session. Semi-structured interview questions included:
Situational maps are strategies for describing the elements in a situation and exploring their interrelations. There are different types of situational maps, including messy and ordered situational maps and relational maps. To create a messy map, the researcher randomly places all related elements on a sheet of paper. This allows researchers to observe elements regardless of their position in a particular situation. A free flow of mind and reflecting on various parts and roles of a factor in a situation enables the researcher to discover different, unknown, and unexpected dimensions.
Data collection and analysis
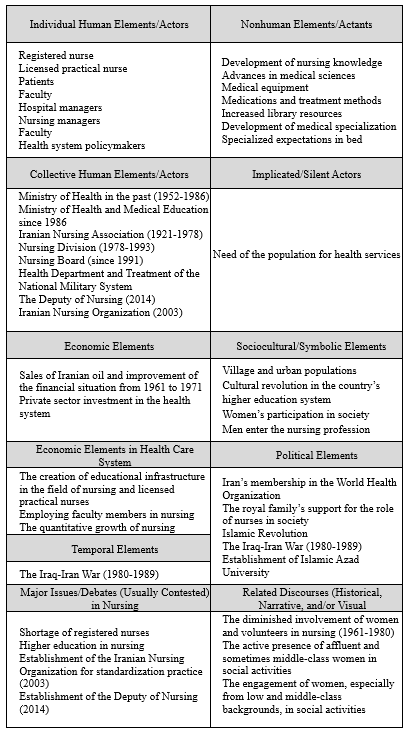
The data analysis was conducted using MAXQDA version 10. The recorded interviews were initially transcribed. Then, to gain profound insights into the statements of participants, the transcripts of the interviews were carefully reviewed multiple times. After writing the initial codes, meaning units were extracted. The sub-categories and main categories were identified by comparing codes based on their differences and similarities. In a situational-ordered map, categories are all elements. This map contains an open-ended list that varies based on the dynamics of each research project. Table 2 shows an instance of the organized map of changes in nursing organizations and nursing role development.
After this analysis, by drawing a map of social worlds and arenas, the main statements related to nursing role development were analyzed (Figure 1).
According to Lincoln and Guba, credibility could be established by allocating sufficient time to each interview, prolonged engagement, and member check. We also asked 2 members of the school of nursing, who were experts in qualitative studies, to check the quality of interviews, coding, and categories to ensure confirmability. For the purpose of dependability, all stages of the study were reported in detail. Finally, transferability was established by maximum variation sampling. Additional interviews were conducted with eyewitnesses to verify the data derived from original historical documents. Secondary sources were also compared with other available sources.
Results
This study aimed to explore the life cycles of nursing organizations and the health care system in Iran based on the Clark situational analysis approach. In addition to investigating the life cycle of organizations, this paper analyzed changes in the role of nurses over the last century.
To shed further light on the situation over time, the researcher used a multi-layered chart. In this chart, the horizontal axis shows the year, and the vertical axis represents the organizational development index in each layer. Also, 7-step trends are marked with letters A to G (black and white columns). Each letter indicates a map of concepts related to the role of nursing. Identify these concepts for each time point, the researcher first drew messy situational maps and then analyzed the Clark map. Also, there were about 15 open codes in this study (Table 3).
Situational map
Therefore, a host of physicians were required to expand services to the villages and alleviate the pressure induced by the Iran-Iraq war crisis (11, 14). Between 1980 and 1989, amid the pressure mounted by society's urgent need for care and medical services, medical education was entrusted with an institution independent of the Ministry of Science. Therefore, in the post-Iran-Iraq war era, the growth of nurses in terms of quantity and experimental development of nursing roles had a major consequence for the nursing profession (15-18). With the establishment of medical science universities and nursing schools, the Ministry of Health and Medical Education (MOHEM) underwent a structural revolution.
Also, private hospitals began to appear in 1991. Medical specialists entered the governmental and political structure of the country, and physicians became the head of all medical universities, national insurance tariffs, and more than 95% of the hospitals. Besides, medical specialists became prominent members of the Health and Treatment Commission of the Islamic Consultative Assembly. This commission was responsible for making legal decisions in support of public health. Under these circumstances, physicians and medical specialists not only enjoyed high income and prestige but also gained political, economic, and social power. As a result, the health care system developed and became mature rapidly. With the growing power of physicians in the macrostructure of the health system, conflicts of interest gradually emerged between the performance and behavior of health system policymakers and the nursing profession (especially in situation G depicted in Figure 2). These conditions suppressed nursing organizations and wielded adverse effects on nursing role development. In this situation, "the unbalanced distribution of financial resources in the health system" was a major challenge.
Unbalanced distribution of financial resources in the health system: According to the Statistical Center of Iran, health expenditures of GDP have been relatively constant over 20 years (1991 to 2011) (19, 20). Therefore, it can be inferred that the health system's focus is primarily on treatment rather than on prevention. This can be seen from the fact that only 5% of the budget was allocated to health and prevention, while the remaining 95% was allocated to treatment. Therefore, the budget allocation highlights the health system's emphasis on treatment rather than on preventative measures. Meanwhile, 1% of direct costs was allocated to nursing services. Nursing Organizations (the educational system of colleges and the Nursing Board) have defined specialized nursing fields. However, no specific position has been described in the organizational chart of the graduates' specialized functions. This could be attributed to the inadequate financial support of health system managers and government from nursing role development in hospitals. In one of the interviews, a participant elaborated on this issue and said:
But due to some conflicts, health care is not as it should be. It is affected by the structure of the Ministry of Health. Now, our main goal is to increase the number of beds. Every year, at least a thousand new hospital beds are added, and so the focus on health promotion declines. We have been permitted to employ 7000 new nurses, but officials argue that this work warrants further investigation. We have explained to everyone in the organization that no one supports us, but they say it is not within their authority.
2- B) The growth of nursing organizations (1961-1978(: In the wake of 2 scientific congresses of the INA held in 1965 and 1975, the nursing role's education was expanded, and nursing education systems were improved (21). Therefore, the INA's performance and activities paved the way for the foundation of Professional Nursing Organizations in Iran (B). This process was associated with the shifting role of nurses from basic and experimental care to scientific and professional care (1961-1978).
2- C, D) Stagnation of the health system and nursing system (1978-1986): As shown in Figure 2, during 1978-1986, there was a relatively straight curve in the health system's structure, including RNs and LPNs. In the wake of the Islamic Revolution and the transformation of the monarchy regime into the Islamic Republic of Iran, a cultural revolution spread in the Iranian structures.
2- E, F) The expansion of nursing organizations in parallel with the advancement of the nursing role: The Nursing Board, the Professional Nurses Associations, the Iranian Nursing Organization (INO), and the Deputy of Nursing were established from 1989 to 2014. In keeping with the concept of "expanding nursing organizations," after the transformation of nursing schools and institutions into colleges, the structure of nursing education changed. The expansion of postgraduate nursing education, medical specialization, clinically specialized expectations, and medical technology development persisted in the early nineties. Therefore, nurses were able to obtain master's and PhD degrees in Iran (16), which reflected advancement in the structure of organizations, nursing education, and the role of graduated nurses. This manifests a relatively remarkable scientific progress in training general and specialized nursing roles, as well as the maturity of the OLC. However, the nursing profession struggled with role ambiguity (G). First, we described the concept of "dispersed power in nursing organizations," and they analyzed "role ambiguity in nursing profession."
2- G) Dispersed power in professional nursing organizations along with role ambiguity in nursing: Power in a system comes from duty, hierarchy, and sometimes centrality. The analysis of the social world map shows that although nursing organizations have expanded in the last decade, the nursing profession has faced the risk of "power dispersion in the nursing organizations" since 2014. The Iranian Nursing Organization (established in 2003) is independent of the MOHEM and makes autonomous decisions. Although the establishment of the Deputy of Nursing, an organization in the government's managerial structure, is unprecedented in the world, the Deputy of Nursing (founded in 2014) is at its nascent stage as a legislative organization. Therefore, it does function independently in its organizational interactions with other nursing systems. On the other hand, the overlapping roles and functions of INO and the Deputy of Nursing can create challenges for managers in decision-making.
The most significant achievement of the Nursing Board has been the addition of PhD courses to the nursing curriculum, but they still do not know what course of action to take. However, the Nursing Board cannot do anything on its own. They have no connection with the faculty and the nursing system, and no meeting has been held with the representatives of these organizations. We just have to advance the system, and I no longer see any integration between the faculties, the board, and other bodies most of the time. These bodies may inadvertently contradict each other’s measures. (Participant 8)
The Nursing Board is a subsystem of the Ministry of Health's educational deputyship, which plays an academic and advisory role in policymaking. In recent years, the Nursing Board has been split into 3 national domains to distribute its decision-making power. Therefore, the reduced decision-making power of managers has diminished the integrated policymaking of nursing organizations. Thus, scenario G, which aims to reconstruct the environment for new roles and role-play, has encountered the serious challenge of "ambiguous role of nurses."
Role ambiguity of nurses:
Following the development of nursing education, the surfeit of nurses with postgraduate degrees mounted a new challenge called "role ambiguity at all nursing levels and hierarchies" because the hospital structure was not prepared to accommodate specialized nurses. This challenge is due to the dispersed power of nursing organizations and weak interaction of the health system during the development of nursing roles. Such organizational behaviors can undermine basic care through non-nursing activities, such as accounting and secretary, that are assigned by RN to the nurses, leading to the complexities of care and treatment, along with the specialization of medical sciences, electronic health system, an excess of nurses with master's degrees in 13 different fields without a defined job descriptions and positions in the clinical settings, etc. This multifaceted challenge and low quality of care and safety for clients have increased the workload of Iranian nurses.
A nurse working in the surgery ward has to prepare up to 8 patients for the operating room and provide postoperative care during the work shift. With this busy schedule, you would not have time for things such as in-job training, measuring blood sugar, or recording the type of dressing in the medical records. Therefore, nurses are under great pressure. Under these circumstances, you have to sacrifice some roles. (Participant 20, a neonatal intensive care unit [NICU] nurse)
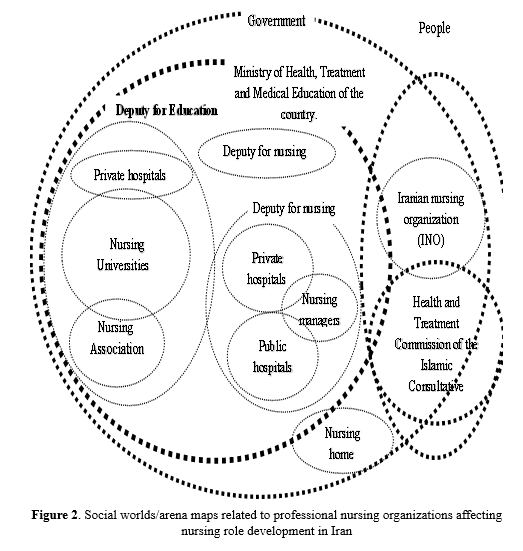
Social worlds/Arenas maps
Social worlds/arenas maps examine the individual and collective actions of people in current discourses. Social worlds/arena maps outline the major collective groups and the areas of commitment they are engaged in (27). Figure 2 shows the nursing organizations in Iran. Depending on their positions and roles in the system, these organizations may have varying degrees of power and influence. Currently, MOHEM is the main obstacle to the provision of the nursing system's financial resources. This issue has been particularly highlighted in the last 10 years with the consolidation of power in medicine. Independent trade :union:s (with official permission from the Ministry of Interior), including INO and the Nursing Home, are beyond the chart and organizations supervised by the MOHEM. Therefore, nurses can exploit these supporting systems to gain a greater share of health system resources. Also, the role of the Deputy of Nursing is limited to a managerial position.
Positional map
These positions have been developed around differences and conflicts over a wide range of issues. The key roles in the situational analysis of nursing organizations in Iran over the last hundred years are as follows: In scenario B, INA has been responsible for policymaking in nursing. Since physicians and nurses have equal powers under this scenario, graduated nurses and nursing organizations have been developed in parallel. Scenarios E and F, along with the expansion of organizations, reflect the first and second stages of role development (defining and explaining the role and teaching specialized nursing in colleges). In scenario G, a significant conflict of interest between nursing organizations and MOHEM has reduced inter-organizational interactions. As a result, the integrated and coherent actions of nursing organizations have declined in the last 6 years (2015-2021).
Discussion
The present study aimed to analyze the situation of nursing organizations and the health system in the wake of nursing role development over the past century in Iran. The results showed that the presence of nursing managers and policymakers is essential in making major decisions, especially in organizations in charge of allocating budgets and financial resources, to develop the role of nursing.
In general, the nursing role has grown and developed in the OLC (9). Still, the nursing role has become ambiguous with the dispersion of power in professional nursing organizations. The current situation does not showcase the life cycle development of the health system. Two key points must be heeded when comparing these processes. First, the OLC of nursing in Iran usually follows the health system's life cycle (except for the systemic stagnation in 2 scenarios from 1978 to 1989). Second, the development of general and specialized nursing roles has been accelerated following changes in professional nursing organizations.
Despite the general correspondence of stages of the OLC in Iran and other countries, they differ in time trends. In most countries, professional nursing organizations were set up with the mission (professional, governmental, legal, or :union:) to turn individual voices into a collective one and make effective decisions. In the United States, for example, with the rising number of nurses in the 1890s and the establishment of 2 professional associations, this trend expanded into some other states (2, 22). However, the first Iranian nursing association was founded in 1951 (about 60 years later). The main role of nursing associations is to issue work permits for nurses, but the Iranian nurses association did not assume such a responsibility because nurses needed no work permit except for a degree certificate. At that time, this legal permission marked a significant achievement for the nursing profession because women had limited political power (5, 23). A number of social factors at that time, such as the limited participation of women in the community and the small number of volunteer nurses, may explain this situation (11). This was the case until 2003 when the INO was established (24). Therefore, nurses obtained a dedicated number for the first time, though they did not require it in Iran. In 2016, the Ministry of Health issued a professional qualification certificate for nurses. However, due to the plethora of working nurses and administrative problems, it was constrained to nurses working over the last 5 years. The certificate was issued by the official management system of the ministry rather than a professional organization.
The present study demonstrates that although the Iranian nursing education system has been developed in B, E, and F scenarios, scenario G has encountered the serious challenge of "role ambiguity and confusion" at different nursing levels (from LPNs to RNs and postgraduate nurses). This role ambiguity is chiefly due to the dispersion of power in professional nursing organizations, reduced decision-making power of nurse managers, inadequate financial support of the health system, and unbalanced economic distribution and power in the health system.
Another reason could be the legislative and legal gap in the nursing profession. It has been over a decade since legal and nursing organizations in Iran (as shown in Figure 1) established standards and regulatory bodies. Organizational structure and specialized nursing departments have been formed over this period. With the changing approach of the health system and the specialization of medical sciences worldwide, specialized nursing roles expanded in 1970 in parallel with the expansion of professional nursing organizations (25, 26). At that time, postgraduate nursing programs were being developed, and nursing roles were general in nature. From 2008 onward, specialized nursing roles were integrated into nursing curricula. In light of these changes in the educational system, professional organizations drafted the first editions of 2 standard books called nursing services (2008) and job descriptions of different nursing levels/hierarchies (2018). Unfortunately, nurses have no legal and financial leverage or support to enforce such job descriptions. Therefore, nurses face a structural obstacle to the development of their role. However, developed countries, such as the United Kingdom, the United States, and Australia, developed legislative, regulatory, budgeting, and standardization structures in nursing more than half a century ago (8, 27-29), and their professional organizations have fueled this development.
The last reason for role ambiguity might be the self-reported accreditation made by the systems and the assessment of employees' professional competence by the health system. The Organization for Economic Co-operation and Development (OECD) has recently called for the separate role of professional organizations, advocating a clear separation of powers to minimize conflicts of interest and resource wastage in organizations (30). Scenario G manifests a significant conflict of interest between the health system and nurses in terms of financial and resource distribution in Iran, which has led to the ambiguous role of organizations and minimized interactions between the systems. Therefore, to define an exact organizational role in the health system and the nursing profession and nurture cohesion and cooperation within the nursing profession, we need strategies to reduce conflicts of interest between nurses and physicians. The payment system, health insurance, financial system, and accreditation mechanism in countries such as the United Kingdom, the United States, Australia, and Thailand are in accordance with their governmental and public conditions (13, 19).
This study had some limitations. It was very difficult to get permission to interview high-level managers of the health system, and interviews were not possible. Also, some of the library archive documents could not be read due to their high historical age, and the documents were distorted, so the researcher did not use them.
Conclusion
It is essential to have nursing managers and policymakers at the macro-level decision-making, especially in organizations in charge of budget allocation and financial resources, to develop the role of nursing. Therefore, nursing leaders need to foster their interaction and diplomacy to be able to strike a balance between the micro-, middle, and macrostructures of nursing.
Acknowledgement
We would like to thank all nurses who offered their valuable time to the research team. This study is part of a PhD dissertation on nursing by the first author and was approved and supported financially by Tarbiat Modares University's Research Deputy. All authors would like to express their gratitude to Tarbiat Modares University.
Funding sources
This study was financially supported by Tarbiat Modares University, Tehran, Iran.
Ethical statement
This study was approved by the Ethics Committee of Tarbiat Modares University (code: 1397.027). Written informed consent for participation in the study was obtained from the participants after explaining the purpose and the method of the study. Participants were also assured of the confidentiality of the information and audio files, and it was stated that they could withdraw from the study at any stage with no harm.
Conflicts of interest
The authors declare that there are no conflicts of interest in the publication of this article.
Author contributions
K.M., E.M., Z.V., and S.R.M. contributed to the design and implementation of the research, the analysis of the results, and the writing of the manuscript.
The research community of this study included registered nurses (RNs) and licensed practical nurses (LPNs) in health care centers and clinics, instructors of nursing schools, and nurse managers. Some repeated patterns emerged after 17 interviews, and data saturation was achieved after 24 interviews. However, we conducted 33 interviews to ensure the sufficiency of data. Data were collected through in-depth semi-structured interviews with 33 Iranian nurses. The location of the interviews was different based on the interests of the participants (at work, hospital, home, etc.) (Table 1). The sources of data collection include interviews, analysis of documents at Dr Madah Association and the National Library of Iran, statistics, government documents, international reports, and historical articles about nursing organizations, as well as reports on the role of LPNs and RNs. Participants were selected using purposive sampling from September 2018 to February 2021. Written consent was obtained from the participants. The interviews, conducted by the first author, lasted 30 to 60 minutes per session. Semi-structured interview questions included:
- What is the current status of nursing organizations? How do you evaluate changes in the role of nursing organizations in Iran? What improvements have you noticed?
- What factors may influence the changes you mentioned?
- What are the concerns about the role of nursing organizations? What are the consequences of changes in the role of nursing organizations?
- How do nursing managers act in the process of changing the nursing role?
Situational maps are strategies for describing the elements in a situation and exploring their interrelations. There are different types of situational maps, including messy and ordered situational maps and relational maps. To create a messy map, the researcher randomly places all related elements on a sheet of paper. This allows researchers to observe elements regardless of their position in a particular situation. A free flow of mind and reflecting on various parts and roles of a factor in a situation enables the researcher to discover different, unknown, and unexpected dimensions.
Data collection and analysis
The data analysis was conducted using MAXQDA version 10. The recorded interviews were initially transcribed. Then, to gain profound insights into the statements of participants, the transcripts of the interviews were carefully reviewed multiple times. After writing the initial codes, meaning units were extracted. The sub-categories and main categories were identified by comparing codes based on their differences and similarities. In a situational-ordered map, categories are all elements. This map contains an open-ended list that varies based on the dynamics of each research project. Table 2 shows an instance of the organized map of changes in nursing organizations and nursing role development.
After this analysis, by drawing a map of social worlds and arenas, the main statements related to nursing role development were analyzed (Figure 1).
|
Table 1. Demographic characteristics of the participants
 |
|
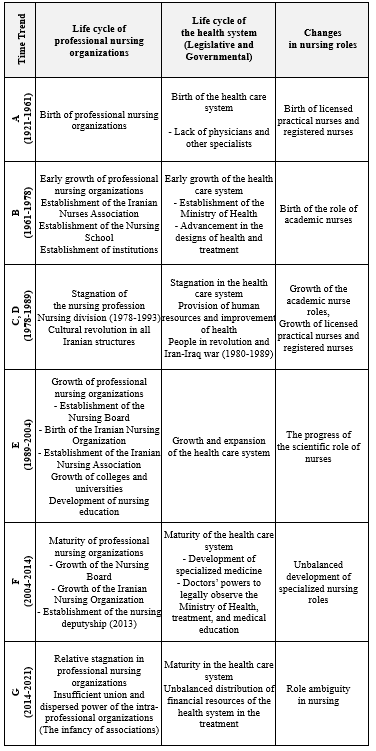
Table 2. The trend of changes in the role of nurses and professional nursing organizations in Iran over the past century according to the clarke ordered-situational map
 |
Results
This study aimed to explore the life cycles of nursing organizations and the health care system in Iran based on the Clark situational analysis approach. In addition to investigating the life cycle of organizations, this paper analyzed changes in the role of nurses over the last century.
To shed further light on the situation over time, the researcher used a multi-layered chart. In this chart, the horizontal axis shows the year, and the vertical axis represents the organizational development index in each layer. Also, 7-step trends are marked with letters A to G (black and white columns). Each letter indicates a map of concepts related to the role of nursing. Identify these concepts for each time point, the researcher first drew messy situational maps and then analyzed the Clark map. Also, there were about 15 open codes in this study (Table 3).
|
Table 3. The situational map of the life cycles of professional nursing organizations and the health care system in parallel with changes in the role of nurses in the last century in Iran
 |
- Life cycle of the health care system (Macrosystem)
Therefore, a host of physicians were required to expand services to the villages and alleviate the pressure induced by the Iran-Iraq war crisis (11, 14). Between 1980 and 1989, amid the pressure mounted by society's urgent need for care and medical services, medical education was entrusted with an institution independent of the Ministry of Science. Therefore, in the post-Iran-Iraq war era, the growth of nurses in terms of quantity and experimental development of nursing roles had a major consequence for the nursing profession (15-18). With the establishment of medical science universities and nursing schools, the Ministry of Health and Medical Education (MOHEM) underwent a structural revolution.
Also, private hospitals began to appear in 1991. Medical specialists entered the governmental and political structure of the country, and physicians became the head of all medical universities, national insurance tariffs, and more than 95% of the hospitals. Besides, medical specialists became prominent members of the Health and Treatment Commission of the Islamic Consultative Assembly. This commission was responsible for making legal decisions in support of public health. Under these circumstances, physicians and medical specialists not only enjoyed high income and prestige but also gained political, economic, and social power. As a result, the health care system developed and became mature rapidly. With the growing power of physicians in the macrostructure of the health system, conflicts of interest gradually emerged between the performance and behavior of health system policymakers and the nursing profession (especially in situation G depicted in Figure 2). These conditions suppressed nursing organizations and wielded adverse effects on nursing role development. In this situation, "the unbalanced distribution of financial resources in the health system" was a major challenge.
Unbalanced distribution of financial resources in the health system: According to the Statistical Center of Iran, health expenditures of GDP have been relatively constant over 20 years (1991 to 2011) (19, 20). Therefore, it can be inferred that the health system's focus is primarily on treatment rather than on prevention. This can be seen from the fact that only 5% of the budget was allocated to health and prevention, while the remaining 95% was allocated to treatment. Therefore, the budget allocation highlights the health system's emphasis on treatment rather than on preventative measures. Meanwhile, 1% of direct costs was allocated to nursing services. Nursing Organizations (the educational system of colleges and the Nursing Board) have defined specialized nursing fields. However, no specific position has been described in the organizational chart of the graduates' specialized functions. This could be attributed to the inadequate financial support of health system managers and government from nursing role development in hospitals. In one of the interviews, a participant elaborated on this issue and said:
But due to some conflicts, health care is not as it should be. It is affected by the structure of the Ministry of Health. Now, our main goal is to increase the number of beds. Every year, at least a thousand new hospital beds are added, and so the focus on health promotion declines. We have been permitted to employ 7000 new nurses, but officials argue that this work warrants further investigation. We have explained to everyone in the organization that no one supports us, but they say it is not within their authority.
- Life cycle of nursing organization (Mesosystem)
2- B) The growth of nursing organizations (1961-1978(: In the wake of 2 scientific congresses of the INA held in 1965 and 1975, the nursing role's education was expanded, and nursing education systems were improved (21). Therefore, the INA's performance and activities paved the way for the foundation of Professional Nursing Organizations in Iran (B). This process was associated with the shifting role of nurses from basic and experimental care to scientific and professional care (1961-1978).
2- C, D) Stagnation of the health system and nursing system (1978-1986): As shown in Figure 2, during 1978-1986, there was a relatively straight curve in the health system's structure, including RNs and LPNs. In the wake of the Islamic Revolution and the transformation of the monarchy regime into the Islamic Republic of Iran, a cultural revolution spread in the Iranian structures.
2- E, F) The expansion of nursing organizations in parallel with the advancement of the nursing role: The Nursing Board, the Professional Nurses Associations, the Iranian Nursing Organization (INO), and the Deputy of Nursing were established from 1989 to 2014. In keeping with the concept of "expanding nursing organizations," after the transformation of nursing schools and institutions into colleges, the structure of nursing education changed. The expansion of postgraduate nursing education, medical specialization, clinically specialized expectations, and medical technology development persisted in the early nineties. Therefore, nurses were able to obtain master's and PhD degrees in Iran (16), which reflected advancement in the structure of organizations, nursing education, and the role of graduated nurses. This manifests a relatively remarkable scientific progress in training general and specialized nursing roles, as well as the maturity of the OLC. However, the nursing profession struggled with role ambiguity (G). First, we described the concept of "dispersed power in nursing organizations," and they analyzed "role ambiguity in nursing profession."
2- G) Dispersed power in professional nursing organizations along with role ambiguity in nursing: Power in a system comes from duty, hierarchy, and sometimes centrality. The analysis of the social world map shows that although nursing organizations have expanded in the last decade, the nursing profession has faced the risk of "power dispersion in the nursing organizations" since 2014. The Iranian Nursing Organization (established in 2003) is independent of the MOHEM and makes autonomous decisions. Although the establishment of the Deputy of Nursing, an organization in the government's managerial structure, is unprecedented in the world, the Deputy of Nursing (founded in 2014) is at its nascent stage as a legislative organization. Therefore, it does function independently in its organizational interactions with other nursing systems. On the other hand, the overlapping roles and functions of INO and the Deputy of Nursing can create challenges for managers in decision-making.
The most significant achievement of the Nursing Board has been the addition of PhD courses to the nursing curriculum, but they still do not know what course of action to take. However, the Nursing Board cannot do anything on its own. They have no connection with the faculty and the nursing system, and no meeting has been held with the representatives of these organizations. We just have to advance the system, and I no longer see any integration between the faculties, the board, and other bodies most of the time. These bodies may inadvertently contradict each other’s measures. (Participant 8)
The Nursing Board is a subsystem of the Ministry of Health's educational deputyship, which plays an academic and advisory role in policymaking. In recent years, the Nursing Board has been split into 3 national domains to distribute its decision-making power. Therefore, the reduced decision-making power of managers has diminished the integrated policymaking of nursing organizations. Thus, scenario G, which aims to reconstruct the environment for new roles and role-play, has encountered the serious challenge of "ambiguous role of nurses."
Role ambiguity of nurses:
Following the development of nursing education, the surfeit of nurses with postgraduate degrees mounted a new challenge called "role ambiguity at all nursing levels and hierarchies" because the hospital structure was not prepared to accommodate specialized nurses. This challenge is due to the dispersed power of nursing organizations and weak interaction of the health system during the development of nursing roles. Such organizational behaviors can undermine basic care through non-nursing activities, such as accounting and secretary, that are assigned by RN to the nurses, leading to the complexities of care and treatment, along with the specialization of medical sciences, electronic health system, an excess of nurses with master's degrees in 13 different fields without a defined job descriptions and positions in the clinical settings, etc. This multifaceted challenge and low quality of care and safety for clients have increased the workload of Iranian nurses.
A nurse working in the surgery ward has to prepare up to 8 patients for the operating room and provide postoperative care during the work shift. With this busy schedule, you would not have time for things such as in-job training, measuring blood sugar, or recording the type of dressing in the medical records. Therefore, nurses are under great pressure. Under these circumstances, you have to sacrifice some roles. (Participant 20, a neonatal intensive care unit [NICU] nurse)
Social worlds/Arenas maps
Social worlds/arenas maps examine the individual and collective actions of people in current discourses. Social worlds/arena maps outline the major collective groups and the areas of commitment they are engaged in (27). Figure 2 shows the nursing organizations in Iran. Depending on their positions and roles in the system, these organizations may have varying degrees of power and influence. Currently, MOHEM is the main obstacle to the provision of the nursing system's financial resources. This issue has been particularly highlighted in the last 10 years with the consolidation of power in medicine. Independent trade :union:s (with official permission from the Ministry of Interior), including INO and the Nursing Home, are beyond the chart and organizations supervised by the MOHEM. Therefore, nurses can exploit these supporting systems to gain a greater share of health system resources. Also, the role of the Deputy of Nursing is limited to a managerial position.
Positional map
These positions have been developed around differences and conflicts over a wide range of issues. The key roles in the situational analysis of nursing organizations in Iran over the last hundred years are as follows: In scenario B, INA has been responsible for policymaking in nursing. Since physicians and nurses have equal powers under this scenario, graduated nurses and nursing organizations have been developed in parallel. Scenarios E and F, along with the expansion of organizations, reflect the first and second stages of role development (defining and explaining the role and teaching specialized nursing in colleges). In scenario G, a significant conflict of interest between nursing organizations and MOHEM has reduced inter-organizational interactions. As a result, the integrated and coherent actions of nursing organizations have declined in the last 6 years (2015-2021).
Discussion
The present study aimed to analyze the situation of nursing organizations and the health system in the wake of nursing role development over the past century in Iran. The results showed that the presence of nursing managers and policymakers is essential in making major decisions, especially in organizations in charge of allocating budgets and financial resources, to develop the role of nursing.
In general, the nursing role has grown and developed in the OLC (9). Still, the nursing role has become ambiguous with the dispersion of power in professional nursing organizations. The current situation does not showcase the life cycle development of the health system. Two key points must be heeded when comparing these processes. First, the OLC of nursing in Iran usually follows the health system's life cycle (except for the systemic stagnation in 2 scenarios from 1978 to 1989). Second, the development of general and specialized nursing roles has been accelerated following changes in professional nursing organizations.
Despite the general correspondence of stages of the OLC in Iran and other countries, they differ in time trends. In most countries, professional nursing organizations were set up with the mission (professional, governmental, legal, or :union:) to turn individual voices into a collective one and make effective decisions. In the United States, for example, with the rising number of nurses in the 1890s and the establishment of 2 professional associations, this trend expanded into some other states (2, 22). However, the first Iranian nursing association was founded in 1951 (about 60 years later). The main role of nursing associations is to issue work permits for nurses, but the Iranian nurses association did not assume such a responsibility because nurses needed no work permit except for a degree certificate. At that time, this legal permission marked a significant achievement for the nursing profession because women had limited political power (5, 23). A number of social factors at that time, such as the limited participation of women in the community and the small number of volunteer nurses, may explain this situation (11). This was the case until 2003 when the INO was established (24). Therefore, nurses obtained a dedicated number for the first time, though they did not require it in Iran. In 2016, the Ministry of Health issued a professional qualification certificate for nurses. However, due to the plethora of working nurses and administrative problems, it was constrained to nurses working over the last 5 years. The certificate was issued by the official management system of the ministry rather than a professional organization.
The present study demonstrates that although the Iranian nursing education system has been developed in B, E, and F scenarios, scenario G has encountered the serious challenge of "role ambiguity and confusion" at different nursing levels (from LPNs to RNs and postgraduate nurses). This role ambiguity is chiefly due to the dispersion of power in professional nursing organizations, reduced decision-making power of nurse managers, inadequate financial support of the health system, and unbalanced economic distribution and power in the health system.
Another reason could be the legislative and legal gap in the nursing profession. It has been over a decade since legal and nursing organizations in Iran (as shown in Figure 1) established standards and regulatory bodies. Organizational structure and specialized nursing departments have been formed over this period. With the changing approach of the health system and the specialization of medical sciences worldwide, specialized nursing roles expanded in 1970 in parallel with the expansion of professional nursing organizations (25, 26). At that time, postgraduate nursing programs were being developed, and nursing roles were general in nature. From 2008 onward, specialized nursing roles were integrated into nursing curricula. In light of these changes in the educational system, professional organizations drafted the first editions of 2 standard books called nursing services (2008) and job descriptions of different nursing levels/hierarchies (2018). Unfortunately, nurses have no legal and financial leverage or support to enforce such job descriptions. Therefore, nurses face a structural obstacle to the development of their role. However, developed countries, such as the United Kingdom, the United States, and Australia, developed legislative, regulatory, budgeting, and standardization structures in nursing more than half a century ago (8, 27-29), and their professional organizations have fueled this development.
The last reason for role ambiguity might be the self-reported accreditation made by the systems and the assessment of employees' professional competence by the health system. The Organization for Economic Co-operation and Development (OECD) has recently called for the separate role of professional organizations, advocating a clear separation of powers to minimize conflicts of interest and resource wastage in organizations (30). Scenario G manifests a significant conflict of interest between the health system and nurses in terms of financial and resource distribution in Iran, which has led to the ambiguous role of organizations and minimized interactions between the systems. Therefore, to define an exact organizational role in the health system and the nursing profession and nurture cohesion and cooperation within the nursing profession, we need strategies to reduce conflicts of interest between nurses and physicians. The payment system, health insurance, financial system, and accreditation mechanism in countries such as the United Kingdom, the United States, Australia, and Thailand are in accordance with their governmental and public conditions (13, 19).
This study had some limitations. It was very difficult to get permission to interview high-level managers of the health system, and interviews were not possible. Also, some of the library archive documents could not be read due to their high historical age, and the documents were distorted, so the researcher did not use them.
Conclusion
It is essential to have nursing managers and policymakers at the macro-level decision-making, especially in organizations in charge of budget allocation and financial resources, to develop the role of nursing. Therefore, nursing leaders need to foster their interaction and diplomacy to be able to strike a balance between the micro-, middle, and macrostructures of nursing.
Acknowledgement
We would like to thank all nurses who offered their valuable time to the research team. This study is part of a PhD dissertation on nursing by the first author and was approved and supported financially by Tarbiat Modares University's Research Deputy. All authors would like to express their gratitude to Tarbiat Modares University.
Funding sources
This study was financially supported by Tarbiat Modares University, Tehran, Iran.
Ethical statement
This study was approved by the Ethics Committee of Tarbiat Modares University (code: 1397.027). Written informed consent for participation in the study was obtained from the participants after explaining the purpose and the method of the study. Participants were also assured of the confidentiality of the information and audio files, and it was stated that they could withdraw from the study at any stage with no harm.
Conflicts of interest
The authors declare that there are no conflicts of interest in the publication of this article.
Author contributions
K.M., E.M., Z.V., and S.R.M. contributed to the design and implementation of the research, the analysis of the results, and the writing of the manuscript.
Type of study: Original Article |
Subject:
Nursing
References
1. Fitzpatrick JJ, Alfes CM. Nurse Leadership and Management: Foundations for Effective Administration. New York: Springer Publishing Company; 2022. [View at Publisher] [DOI] [Google Scholar]
2. Vana PK, Tazbir J. Kelly Vana's nursing leadership and management. 4th ed. USA: wiley Blackwell; 2021. [View at Publisher] [Google Scholar]
3. Mosca L, Gianecchini M, Campagnolo D. Organizational life cycle models: a design perspective. J Org Design. 2021;10(1):3-18. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Angeles A, Perez-Encinas A, Villanueva CE. Characterizing organizational lifecycle through strategic and structural flexibility: Insights from MSMEs in Mexico. Glob J Flex Syst Manag. 2022;23(2):271-90. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Masters K. Role development in professional nursing practice. US: Jones & Bartlett Learning; 2018. [View at Publisher] [Google Scholar]
6. WHO. State of the world's nursing 2020: investing in education, jobs and leadership. Geneva: WHO; 2020. [View at Publisher] [Google Scholar]
7. Miri Kh. The Development Of Professional Role Of Nurses In Iran With the Situation Analysis Approach. Tehran: Tarbiat Modares University; 2021 (Ph.D thesis).
8. Benton DC, Thomas K, Damgaard G, Masek SM, Brekken SA. Exploring the differences between regulatory bodies, professional associations, and trade :union:s: An integrative review. Journal of Nursing Regulation. 2017;8(3):4-11. [View at Publisher] [DOI] [Google Scholar]
9. Weiss SA, Tappen RM, Grimley K. Essentials of nursing leadership & management. 7th ed. Philadelphia: FA Davis; 2019. [View at Publisher] [Google Scholar]
10. Barasteh S, Rassouli M, Karimirad MR, Ebadi A. Future challenges of nursing in health system of Iran. Front Public Health. 2021;9:676160. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Sharafi S, Cheraghi MA, Nasiri A, Mahmoudirad G. Diplomatic activities of Iranian Nursing Organization: A qualitative study. Nurs Forum. 2021;56(3):604-11. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Clarke AE, Friese C, Washburn RS. Situational analysis: Grounded theory after the interpretive turn. 2th ed. California: Sage Publications; 2018. [View at Publisher] [DOI] [Google Scholar]
13. Mosadeghrad AM, Rahimi-Tabar P. Health system governance in Iran: A comparative study. Razi Journal of Medical Sciences (RJMS). 2019;26(9):10-28. [View at Publisher] [DOI] [Google Scholar]
14. Firouzkouhi M, Zargham-Boroujeni A, Nouraei M, Rahnama M, Babaiepur M. The effects of imposed war on Iran's nursing: A historical research. Journal of Military Medicine. 2015;17(3):127-36. [View at Publisher] [Google Scholar]
15. Miri K, Sabbaghi M, Mazlum SR, Namazinia M. The trend of change in the role of pre-hospital emergency medical services in Iran’s healthcare system: a situational analysis. BMC Emerg Med. 2023;23(1):99. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Khomeiran RT, Deans C. Nursing education in Iran: Past, present, and future. Nurse education today. 2007;27(7):708-14. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Tsou P, Shih J, Ho M-J. A comparative study of professional and interprofessional values between health professional associations. Journal of interprofessional care. 2015;29(6):628-33. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Ahmadi Chenari H, Zakerimoghadam M, Baumann SL. Nursing in Iran: Issues and challenges. Nursing Science Quarterly. 2020;33(3):264-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Mehrolhasani M, Yazdi Feyzabadi V, Oroomiei N, Seyfaddini R, Mirzaei S. Comparative Study of Health Systems of Liberal, Social, and Mixed Countries Based on CLA Framework. Iranian Journal of Epidemiology (IRJE). 2018;13:14-26. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Rahimisadegh R, Mehrolhassani MH, Jafari Sirizi M, Noori Hekmat S. The analysis of National Health Accounts and financial communications network in Iran health insurance ecosystem. BMC Health Serv Res. 2022;22(1):1552. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Raiesifar A. The Exploration of Academic Nursing History before the Islamic Revolution in Iran: A Historical Study. Tehran: Tehran Unversity of Medical Sciences; 2017.
22. Rafferty AM, Busse R, Zander-Jentsch B, Sermeus W, Bruyneel L, WHO. Strengthening health systems through nursing: Evidence from 14 European countries: World Health Organization. Regional Office for Europe; 2019. 163p. [View at Publisher] [Google Scholar]
23. LaRocco SA. Nursing History for Contemporary Role Development. Nursing History Review. 2018;26(1). [View at Publisher] [DOI] [Google Scholar]
24. Sharafi S, Cheraghi MA, Nasiri A, Mahmoudirad G. Diplomatic activities of Iranian Nursing Organization: A qualitative study. Nurs Forum. 2021;56(3):604-11. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Hämel K, Toso BRGdO, Casanova A, Giovanella L. Advanced practice nursing in primary health care in the Spanish National Health System. Cien Saude Colet. 2020;25(1):303-14. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Irajpour A, Khorasani P, Bagheri M, Eshaghian A, Ziaee ES, Saberi Z, et al. The framework for developing nursing specialist roles in the health care system of Iran. Nurs outlook. 2020;68(1):45-54. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Saputra F. Leadership, Communication, And Work Motivation In Determining The Success Of Professional Organizations. Journal of Law, Politic and Humanities (JLPH). 2021;1(2):59-70. [View at Publisher] [DOI] [Google Scholar]
28. Salvage J, White J. Nursing leadership and health policy: everybody's business. Int Nurs Rev. 2019;66(2):147-50. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Chism LA. The doctor of nursing practice: A guidebook for role development and professional issues. 5th ed. Burlington: Jones & Bartlett Learning; 2021. [View at Publisher] [Google Scholar]
30. Index BL. The Organisation for Economic Co-operation and Development. UN: 2021. p385. [View at Publisher] [DOI] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
