
Volume 22, Issue 2 (6-2025)
J Res Dev Nurs Midw 2025, 22(2): 4-10 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rostami M, Ebadi A, Sharif-Nia H, Shabani F, Ghanei Gheshlagh R. Psychometric evaluation of the Persian version of the Invisible Violence Against Women Questionnaire. J Res Dev Nurs Midw 2025; 22 (2) :4-10
URL: http://nmj.goums.ac.ir/article-1-1970-en.html
URL: http://nmj.goums.ac.ir/article-1-1970-en.html
Psychometric evaluation of the Persian version of the Invisible Violence Against Women Questionnaire



1- Department of Nursing, Asadabad School of Medical Sciences, Asadabad, Iran
2- Nursing Care Research Center, Clinical Sciences Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
3- Psychosomatic Research Center, Mazandaran University of Medical Sciences, Sari, Iran ; Department of Nursing, Amol School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran
4- Cardiovascular Nursing Research Center, Rajaie Cardiovascular Institute, Tehran, Iran
5- Lahore School of Nursing, The University of Lahore, Lahore, Pakistan ; Nursing Department, Biruni University, 34010, Istanbul, Turkey ,rezaghanei30@yahoo.com
2- Nursing Care Research Center, Clinical Sciences Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
3- Psychosomatic Research Center, Mazandaran University of Medical Sciences, Sari, Iran ; Department of Nursing, Amol School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran
4- Cardiovascular Nursing Research Center, Rajaie Cardiovascular Institute, Tehran, Iran
5- Lahore School of Nursing, The University of Lahore, Lahore, Pakistan ; Nursing Department, Biruni University, 34010, Istanbul, Turkey ,
Full-Text [PDF 642 kb]
(578 Downloads)
| Abstract (HTML) (1065 Views)
Discussion
The primary goal of this study was to evaluate the psychometric properties of the Persian version of the Q-IVAW, a tool designed to measure invisible violence against women. The results indicate that this version of the questionnaire is valid and reliable. Although the original version consists of five factors, the Persian version contains four.
The first factor in the Persian version includes items 8, 9, 11, 12, 22, and 23. In the original version, items 8 through 12 were associated with utilitarian sexist behaviors, while items 22 and 23 belonged to the benevolent sexist behaviors factor. We combined these items and labeled the factor “Utilitarian-Benevolent Sexist Behaviors” in the Persian version. Notably, item 10, which addresses the disregard for the economic value of women’s housework, was not assigned to any factor. The highest factor loading was associated with item 11, which refers to women being forced to care for others simply because they are women. The highest mean scores were found for the first four items, all of which relate to utilitarian-sexist behaviors. It seems that Iranian women have experienced the forms of invisible violence reflected in these items more than other forms. According to utilitarianism, actions that lead to happiness or pleasure are endorsed, while those that cause discomfort or harm are rejected (30). Benevolent sexism, a subtler form of sexism, is expressed positively but implicitly suggests women’s lack of competence (31,32). In some contexts, benevolent sexism manifests as a preference for men with benevolent sexist attitudes as romantic partners (33). Additionally, in countries with lower gender equality, the correlation between benevolent sexism and violence against women may be stronger than in more egalitarian countries due to stronger institutional support and punitive measures (34).
The second factor, labeled "Crisis Sexist Behaviors," includes items 3, 4, 5, and 6. In the original version, this factor consisted of 7 items (Items 1 to 7). However, in the Persian version, items 2 and 7 were not assigned to any factor, and item 1 was integrated into another factor. The highest factor loading in this factor was on item 5 (0.756), which refers to giving or promising something to gain a special advantage. The low mean score for items in this factor suggests that Iranian women have experienced these forms of invisible violence less frequently or may not recognize them as such. The third factor, labeled "Coercive Sexist Behavior," includes items 1, 14, and 16. In the Persian version, items 13 and 15 were omitted, as they were considered inconsistent with contemporary social norms in Iran, where women are active in the workforce. Item 1, originally assigned to "Critical Sexist Behavior" in the original version, was included in this factor, as it pertains to the enforcement of the husband’s orders, reflecting coercive control. The highest factor loading was observed for item 14 (0.726), which refers to a husband using physical stature and voice to impose his views. Coercive control is a form of ongoing abuse, involving intimidation, isolation, humiliation, surveillance, and exploitation to deprive individuals of their independence (35,36). If these methods fail, perpetrators may resort to physical and sexual violence (36).
The fourth factor, "Ambivalent Sexist Behavior," consisted of items 17 to 21 in the original version, but items 20 and 21 were not assigned to any factor in the Persian version. These items refer to “withholding information from a partner to avoid unnecessary conflict” and “feigning ignorance to justify harmful behavior.” The remaining three items were categorized as "Ambivalent Sexist Behavior," consistent with the original version. The highest factor loading in this factor was for item 19, which refers to men commenting on women’s appearance and physique in advertisements. The theory of ambivalent sexism posits that sexism manifests as hostility toward women who challenge traditional gender roles and male dominance, and it encompasses both benevolent and hostile sexism. Hostile sexism involves negative attitudes toward women, while benevolent sexism reflects positive attitudes toward traditional women, emphasizing the need to protect and support them (37,38).
This study found a relationship between the mean score of invisible violence and several variables, including the husband’s education and occupation, previous marriages, type of marriage (voluntary or arranged), premarital dating, and monthly income. The original study found that higher violence scores were associated with husbands with higher monthly incomes (23). This was explained by patriarchal norms, which suggest that men with greater financial resources exert more power in relationships (16). However, our study showed the opposite: the highest violence scores were associated with husbands with lower monthly incomes. This discrepancy may be due to the different demographic, cultural, and economic contexts in the two studies, as well as the severe economic challenges in Iran due to international sanctions. In the Persian version, the minimum and maximum mean scores were associated with items 17 and 12. The low mean score for item 17, about husbands making sexual jokes about their wives, may be due to the cultural sensitivity around extramarital affairs in Iran, which is considered a serious offense. This aligns with the findings of Adamczyk and Hayes (2012), who noted fewer extramarital affairs among married Hindus and Muslims compared to their Christian and Jewish counterparts (39). Item 12, which addresses a spouse telling the wife she should be the one to care for children and other loved ones, received the highest score. This reflects the patriarchal structure and gender roles in Iranian society, which allow male violence against women and encourage traditional gender roles (40). This study had several limitations. It focused only on literate women attending health centers in Asadabad, so caution should be taken when generalizing the results to all Iranian women. Additionally, few women visited the health centers with their husbands, which may have influenced their openness in answering questions. Therefore, women without their spouses were not asked to complete the questionnaires.
Conclusion
This methodological study shows that the Persian version of the questionnaire of invisible violence against women is a valid and reliable instrument that can be used to effectively assess this concept in the context of Iranian society. In traditional Iranian society, the term “violence against women” often evokes images of physical and sexual violence that can be proven and tracked based on the visible effects on a woman's body. Therefore, psychological violence is often overlooked. Invisible violence against women in traditional societies is frequently observed but often goes unnoticed because women’s rights are disregarded and they are unaware of these rights. The Persian version of the Q-IVAW, which has undergone psychometric evaluation, is able to measure this concept accurately. It can provide a clear understanding of the prevalence of invisible violence against Iranian women to inform officials, policymakers, researchers and society at large.
Acknowledgement
This study is derived from the research project No. 138, approved by the Ethics Committee of Asadabad School of Medical Sciences. The authors express their gratitude to the Scientific Council and Ethics Committee of Asadabad School of Medical Sciences, as well as to all the women who participated in this study.
Funding sources
This study was funded by the Asadabad School of Medical Sciences. The funding body had no role in the design of the study, data collection, interpretation of the result, or writing the manuscript.
Ethical statement
This study is the result of the project approved by the Asadabad School of Medical Sciences (IR.ASAUMS.REC.1402.028). According to the standards of Ethics in Research, the objectives of the study were explained to the research participants, and written informed consent was obtained to participate in the study. The questionnaires were distributed anonymously, and the participants were assured that their information would be kept confidential. All ethical principles in human research were observed in accordance with the Declaration of Helsinki.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
MR and RGG: manuscript preparation and study conceptualization; MR: data collection and manuscript preparation; RGG and FS: study design; RGG, AE, HSN, FS, and MR: writing-original draft preparation; RGG, AE, HSN, FS, and MR: writing-review and editing; AE and HSN: statistical analysis; RGG: project administration; MR: funding acquisition. All authors read and approved the finall version of the manuscript.
Data availability statement
All data on diagnostic yield analyzed in the current study are presented in the main text or supplementary material.
Full-Text: (227 Views)
Introduction
Violence, in its many forms, is a pattern of behavior that seeks to dominate others-often targeting spouses, children, and elderly family members-through fear, threats, or coercion. It may appear as sexual, physical, economic, or psychological abuse (1). Domestic violence remains a pressing global issue, especially for women. Between 2000 and 2018, one in every three women was estimated to have experienced domestic violence. Alarmingly, nearly one-third of these cases begin or worsen during pregnancy (2,3).
During the COVID-19 pandemic, a meta-analysis reported that 66% of women had faced some form of domestic violence (4). Similar studies have shown high rates in countries like Ethiopia (36.2%) and Brazil (22.4%) (5,6). In Iran, the situation is even more concerning, with a reported prevalence of 66% (7). Among pregnant women, this number is also high-over half (51.5%) have experienced abuse (8). The consequences of domestic violence are deep and far-reaching. It doesn’t just hurt physically-it leaves lasting emotional and psychological scars. Women who experience such violence are at greater risk of mental health conditions, chronic diseases, and substance abuse (9). They are four times more likely to develop anxiety disorders and seven times more likely to suffer from post-traumatic stress disorder compared to women who are not abused (10). Evidence also indicates a link between domestic violence and postpartum depression (11).
However, many women do not-or cannot-speak up. They might visit a health center without showing any clear signs of abuse. They may feel ashamed, unsafe, or unsure of how to ask for help. This makes it incredibly difficult for healthcare providers to recognize what is happening. This form of abuse is often referred to as “invisible violence”-a hidden, yet powerful force that shapes women’s lives (12,13). Invisible violence includes the everyday words, behaviors, and beliefs-often accepted by society-that men might use to control or diminish women (14). It reinforces outdated gender roles, justifies discrimination, and keeps unequal power structures in place (15,16). These subtle forms of harm are frequently overlooked or normalized in the name of tradition or culture (9,17). However, their silence should not be mistaken for harmlessness-invisible violence can escalate into more overt and dangerous forms if not addressed (18,19).
The perception and experience of invisible violence are deeply shaped by cultural values, gender roles, and social norms, as behaviors considered controlling or abusive in one culture may be seen as normal-or even acceptable-in another. Therefore, while the Questionnaire for Invisible Violence Against Women (Q-IVAW), provides a valuable foundation for identifying this form of violence, its effectiveness relies on careful cross-cultural adaptation and validation to ensure that the conceptual, semantic, and contextual meanings are preserved between the original and the target culture. In a context like Iran, where traditional gender expectations and a social silence around family issues may conceal invisible violence, having a precise and culturally sensitive tool to assess this phenomenon is essential. Therefore, the aim of this study was to evaluate the psychometric properties of the Persian version of the Q-IVAW, enabling healthcare professionals in Iran to better identify and respond to this subtle but harmful form of gender-based violence.
Methods
Participants
This cross-sectional study was conducted in the fall and winter of 2023 among 520 married women who visited health centers in Asadabad, a city in Hamadan province in western Iran. The sample size was determined based on guidelines for both exploratory and confirmatory factor analysis. For exploratory factor analysis (EFA), either a total sample size of 200 to 300 participants is considered acceptable, or a subject-to-item ratio of at least 10:1 is recommended (20). For confirmatory factor analysis (CFA), a minimum of 200 participants is generally advised (21). Considering these criteria, a total of 520 women were recruited using a simple non-random sampling method. The participants were included if they met the following criteria: willingness to participate, basic literacy (Ability to read and write), and no known mental or cognitive impairments. Incomplete questionnaires were excluded from the analysis.
Translation process
The translation was carried out using the forward-backward translation method, as recommended by the World Health Organization (WHO). After receiving formal permission from the original developers of the tool, a structured, multi-step translation procedure was implemented to ensure both linguistic accuracy and cultural appropriateness of the Persian version.
Step 1. Forward translation: Two independent bilingual translators, whose native language was Persian and who were fluent in English, were selected. Each translator independently translated the original English version of the Q-IVAW into Persian. One of the translators was a faculty member in the medical sciences, familiar with specialized terminology, while the second translator was chosen specifically for their ability to reflect general, everyday language, as they did not have a medical background.
Step 2. Reconciliation: The research team compared the two translations, discussed any discrepancies, and created a single, reconciled Persian version. The goal of this step was to ensure clarity, cultural relevance, and fidelity to the original concepts.
Step 3. Backward translation: The reconciled Persian version was then independently translated back into English by two bilingual translators who were not aware of the original English version. These translators were fluent in both languages and had not been involved in the forward translation process.
Step 4. Review and comparison: The research team, along with a language expert and a subject matter specialist, compared the two back-translated English versions with the original version of the tool. Any discrepancies were carefully examined to assess semantic, idiomatic, and conceptual equivalence between the versions.
Step 5. Finalization: Based on the review, necessary adjustments were made to the Persian version to ensure that it accurately reflected the meaning and intent of the original items while being linguistically and culturally appropriate for the Iranian context. The finalized Persian version was prepared for face and content validity assessment, followed by psychometric testing (22).
Instruments
Data were collected using a demographic information form and the Persian version of the Q-IVAW. The demographic form included questions about the couple’s age, education level, occupation, medical and marital history, duration of marriage, monthly income, and number of children. The Q-IVAW was originally developed by Dobarrio-Sanz et al. (2022) and consists of five dimensions: crisis sexist behaviors, utilitarian sexist behaviors, coercive sexist behaviors, ambivalent sexist behaviors, and benevolent sexist behaviors. It includes 23 items rated on a 5-point Likert scale, ranging from “never” (Score 1) to “always” (Score 5). The total score is obtained by summing the item scores, resulting in a range from 23 to 115. Higher scores indicate greater levels of perceived invisible violence (23).
Face validity
Face validity refers to the extent to which a questionnaire appears valid to the respondents (24). A questionnaire with good face validity increases the likelihood of respondent cooperation by making it easier to use, appropriately framing the questions, and enhancing clarity. To assess face validity, the Persian version of the Invisible Violence Against Women questionnaire was presented to ten married women. They were asked to read each question aloud and identify any statements that were unclear or confusing. They were also encouraged to suggest alternative wording for any items they found problematic.
Content validity
Content validity refers to the extent to which the questions in a questionnaire cover the content defined in its conceptual scope, as assessed by researchers (24). It ensures that the selected questions are comprehensive and relevant to the construct being measured (25). For content validity, the questionnaire was reviewed by five experts from relevant fields, including a nurse, a midwife, a psychologist, and two methodologists. Each expert evaluated the items in terms of their relevance, clarity, and comprehensiveness. The research team carefully reviewed their feedback and incorporated the suggested revisions into the final version of the questionnaire.
Data analysis
Data were analyzed using SPSS version 26 and AMOS version 26. To evaluate construct validity, both EFA and CFA were conducted. In the EFA, the maximum likelihood extraction method with promax rotation was used to identify the underlying dimensions of the questionnaire. This method helps reduce the number of items while maximizing explained variance and improving reliability (24). The adequacy of the sample was assessed using the Kaiser-Meyer-Olkin (KMO) index, and Bartlett’s test of sphericity was used to evaluate the suitability of the data for factor analysis. A KMO value closer to 1 indicates that the sample is appropriate for factor analysis. Items with communalities greater than 0.2 were retained, and factors were extracted based on eigenvalues greater than 1 (26). Items were assigned to factors if their factor loadings exceeded 0.30 (27).
Confirmatory factor analysis (CFA) was conducted to validate the factor structure derived from exploratory factor analysis. The following indices were used to assess the model fit: Minimum Discrepancy Function by Degrees of Freedom divided (CMIN/DF), Comparative Fit Index (CFI), Incremental Fit Index (IFI), Normed Fit Index (NFI), Non-Normed Fit Index (NNFI), Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), Root Mean Square Residual (RMR), Root Mean Square Error of Approximation (RMSEA). Acceptable values for these indices are as follows: CFI ≥0.95; IFI>0.90, NFI>0.95, NNFI>0.9, GFI>0.95, AGFI>0.80; RMR<0.08, and RMSEA <0.08 (Fair), or ideally <0.06 (28). To assess reliability, both Cronbach’s alpha and McDonald’s omega coefficients were calculated. Values above 0.70 were considered acceptable (26). The test–retest reliability was also examined by re-administering the questionnaire to 30 eligible participants (Mean age: 31.8 ± 9.60 years) after a two-week interval. The intraclass correlation coefficient (ICC) was calculated using a two-way mixed-effects model with absolute agreement. An ICC >0.75 was considered indicative of good stability (29).
Results
This study included 520 women who were referred to health centers. The mean age of the participants was 34.76 years (Standard deviation = 8.48), ranging from 17 to 66 years. The mean age of their husbands was 39.75 years (SD = 8.42), with an age range from 20 to 70 years. On average, the couples had been married for 13.89 years (SD = 8.8). The majority of the women were unemployed, had completed high school, earned an average monthly income, and had two children. Additional details regarding premarital dating, marriage preferences, and previous health or marital history (for both men and women) are provided in Table 1.
Face and content validity
None of the items were changed with regard to face validity. For content validity, items 2 and 7 were rewritten in simpler language to improve comprehension. These two items were not assigned to any factor in the factor analysis.
Construct validity: The results of exploratory factor analysis
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.889, indicating that the sample was suitable for factor analysis. Bartlett’s test for sphericity was significant (Chi-square = 2666.587, DF = 120, p < 0.001), confirming the data were appropriate for structural identification. Exploratory factor analysis (EFA) was conducted using the maximum likelihood method and promax rotation. Four factors were extracted, which together explained 47.17% of the total variance in invisible violence. Seven items (Items 2, 7, 10, 13, 15, 20, and 21) did not load on any factor.
Factor 1: "Utilitarian-Benevolent sexist behavior"
This factor included items 8, 9, 11, 12, 22, and 23, explaining 13.76% of the total variance. Its eigenvalue was 2.203. The internal consistency of this factor, measured by Cronbach’s alpha and McDonald’s omega coefficients, was 0.803 and 0.806, respectively. The ICC for this factor was 0.859 (95% CI: 0.796–0.924). The highest mean scores were found for items 12 (2.66±1.54), 9 (2.19±1.41), 8 (2.18±1.42), and 11 (2.13±1.34).
Violence, in its many forms, is a pattern of behavior that seeks to dominate others-often targeting spouses, children, and elderly family members-through fear, threats, or coercion. It may appear as sexual, physical, economic, or psychological abuse (1). Domestic violence remains a pressing global issue, especially for women. Between 2000 and 2018, one in every three women was estimated to have experienced domestic violence. Alarmingly, nearly one-third of these cases begin or worsen during pregnancy (2,3).
During the COVID-19 pandemic, a meta-analysis reported that 66% of women had faced some form of domestic violence (4). Similar studies have shown high rates in countries like Ethiopia (36.2%) and Brazil (22.4%) (5,6). In Iran, the situation is even more concerning, with a reported prevalence of 66% (7). Among pregnant women, this number is also high-over half (51.5%) have experienced abuse (8). The consequences of domestic violence are deep and far-reaching. It doesn’t just hurt physically-it leaves lasting emotional and psychological scars. Women who experience such violence are at greater risk of mental health conditions, chronic diseases, and substance abuse (9). They are four times more likely to develop anxiety disorders and seven times more likely to suffer from post-traumatic stress disorder compared to women who are not abused (10). Evidence also indicates a link between domestic violence and postpartum depression (11).
However, many women do not-or cannot-speak up. They might visit a health center without showing any clear signs of abuse. They may feel ashamed, unsafe, or unsure of how to ask for help. This makes it incredibly difficult for healthcare providers to recognize what is happening. This form of abuse is often referred to as “invisible violence”-a hidden, yet powerful force that shapes women’s lives (12,13). Invisible violence includes the everyday words, behaviors, and beliefs-often accepted by society-that men might use to control or diminish women (14). It reinforces outdated gender roles, justifies discrimination, and keeps unequal power structures in place (15,16). These subtle forms of harm are frequently overlooked or normalized in the name of tradition or culture (9,17). However, their silence should not be mistaken for harmlessness-invisible violence can escalate into more overt and dangerous forms if not addressed (18,19).
The perception and experience of invisible violence are deeply shaped by cultural values, gender roles, and social norms, as behaviors considered controlling or abusive in one culture may be seen as normal-or even acceptable-in another. Therefore, while the Questionnaire for Invisible Violence Against Women (Q-IVAW), provides a valuable foundation for identifying this form of violence, its effectiveness relies on careful cross-cultural adaptation and validation to ensure that the conceptual, semantic, and contextual meanings are preserved between the original and the target culture. In a context like Iran, where traditional gender expectations and a social silence around family issues may conceal invisible violence, having a precise and culturally sensitive tool to assess this phenomenon is essential. Therefore, the aim of this study was to evaluate the psychometric properties of the Persian version of the Q-IVAW, enabling healthcare professionals in Iran to better identify and respond to this subtle but harmful form of gender-based violence.
Methods
Participants
This cross-sectional study was conducted in the fall and winter of 2023 among 520 married women who visited health centers in Asadabad, a city in Hamadan province in western Iran. The sample size was determined based on guidelines for both exploratory and confirmatory factor analysis. For exploratory factor analysis (EFA), either a total sample size of 200 to 300 participants is considered acceptable, or a subject-to-item ratio of at least 10:1 is recommended (20). For confirmatory factor analysis (CFA), a minimum of 200 participants is generally advised (21). Considering these criteria, a total of 520 women were recruited using a simple non-random sampling method. The participants were included if they met the following criteria: willingness to participate, basic literacy (Ability to read and write), and no known mental or cognitive impairments. Incomplete questionnaires were excluded from the analysis.
Translation process
The translation was carried out using the forward-backward translation method, as recommended by the World Health Organization (WHO). After receiving formal permission from the original developers of the tool, a structured, multi-step translation procedure was implemented to ensure both linguistic accuracy and cultural appropriateness of the Persian version.
Step 1. Forward translation: Two independent bilingual translators, whose native language was Persian and who were fluent in English, were selected. Each translator independently translated the original English version of the Q-IVAW into Persian. One of the translators was a faculty member in the medical sciences, familiar with specialized terminology, while the second translator was chosen specifically for their ability to reflect general, everyday language, as they did not have a medical background.
Step 2. Reconciliation: The research team compared the two translations, discussed any discrepancies, and created a single, reconciled Persian version. The goal of this step was to ensure clarity, cultural relevance, and fidelity to the original concepts.
Step 3. Backward translation: The reconciled Persian version was then independently translated back into English by two bilingual translators who were not aware of the original English version. These translators were fluent in both languages and had not been involved in the forward translation process.
Step 4. Review and comparison: The research team, along with a language expert and a subject matter specialist, compared the two back-translated English versions with the original version of the tool. Any discrepancies were carefully examined to assess semantic, idiomatic, and conceptual equivalence between the versions.
Step 5. Finalization: Based on the review, necessary adjustments were made to the Persian version to ensure that it accurately reflected the meaning and intent of the original items while being linguistically and culturally appropriate for the Iranian context. The finalized Persian version was prepared for face and content validity assessment, followed by psychometric testing (22).
Instruments
Data were collected using a demographic information form and the Persian version of the Q-IVAW. The demographic form included questions about the couple’s age, education level, occupation, medical and marital history, duration of marriage, monthly income, and number of children. The Q-IVAW was originally developed by Dobarrio-Sanz et al. (2022) and consists of five dimensions: crisis sexist behaviors, utilitarian sexist behaviors, coercive sexist behaviors, ambivalent sexist behaviors, and benevolent sexist behaviors. It includes 23 items rated on a 5-point Likert scale, ranging from “never” (Score 1) to “always” (Score 5). The total score is obtained by summing the item scores, resulting in a range from 23 to 115. Higher scores indicate greater levels of perceived invisible violence (23).
Face validity
Face validity refers to the extent to which a questionnaire appears valid to the respondents (24). A questionnaire with good face validity increases the likelihood of respondent cooperation by making it easier to use, appropriately framing the questions, and enhancing clarity. To assess face validity, the Persian version of the Invisible Violence Against Women questionnaire was presented to ten married women. They were asked to read each question aloud and identify any statements that were unclear or confusing. They were also encouraged to suggest alternative wording for any items they found problematic.
Content validity
Content validity refers to the extent to which the questions in a questionnaire cover the content defined in its conceptual scope, as assessed by researchers (24). It ensures that the selected questions are comprehensive and relevant to the construct being measured (25). For content validity, the questionnaire was reviewed by five experts from relevant fields, including a nurse, a midwife, a psychologist, and two methodologists. Each expert evaluated the items in terms of their relevance, clarity, and comprehensiveness. The research team carefully reviewed their feedback and incorporated the suggested revisions into the final version of the questionnaire.
Data analysis
Data were analyzed using SPSS version 26 and AMOS version 26. To evaluate construct validity, both EFA and CFA were conducted. In the EFA, the maximum likelihood extraction method with promax rotation was used to identify the underlying dimensions of the questionnaire. This method helps reduce the number of items while maximizing explained variance and improving reliability (24). The adequacy of the sample was assessed using the Kaiser-Meyer-Olkin (KMO) index, and Bartlett’s test of sphericity was used to evaluate the suitability of the data for factor analysis. A KMO value closer to 1 indicates that the sample is appropriate for factor analysis. Items with communalities greater than 0.2 were retained, and factors were extracted based on eigenvalues greater than 1 (26). Items were assigned to factors if their factor loadings exceeded 0.30 (27).
Confirmatory factor analysis (CFA) was conducted to validate the factor structure derived from exploratory factor analysis. The following indices were used to assess the model fit: Minimum Discrepancy Function by Degrees of Freedom divided (CMIN/DF), Comparative Fit Index (CFI), Incremental Fit Index (IFI), Normed Fit Index (NFI), Non-Normed Fit Index (NNFI), Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), Root Mean Square Residual (RMR), Root Mean Square Error of Approximation (RMSEA). Acceptable values for these indices are as follows: CFI ≥0.95; IFI>0.90, NFI>0.95, NNFI>0.9, GFI>0.95, AGFI>0.80; RMR<0.08, and RMSEA <0.08 (Fair), or ideally <0.06 (28). To assess reliability, both Cronbach’s alpha and McDonald’s omega coefficients were calculated. Values above 0.70 were considered acceptable (26). The test–retest reliability was also examined by re-administering the questionnaire to 30 eligible participants (Mean age: 31.8 ± 9.60 years) after a two-week interval. The intraclass correlation coefficient (ICC) was calculated using a two-way mixed-effects model with absolute agreement. An ICC >0.75 was considered indicative of good stability (29).
Results
This study included 520 women who were referred to health centers. The mean age of the participants was 34.76 years (Standard deviation = 8.48), ranging from 17 to 66 years. The mean age of their husbands was 39.75 years (SD = 8.42), with an age range from 20 to 70 years. On average, the couples had been married for 13.89 years (SD = 8.8). The majority of the women were unemployed, had completed high school, earned an average monthly income, and had two children. Additional details regarding premarital dating, marriage preferences, and previous health or marital history (for both men and women) are provided in Table 1.
Face and content validity
None of the items were changed with regard to face validity. For content validity, items 2 and 7 were rewritten in simpler language to improve comprehension. These two items were not assigned to any factor in the factor analysis.
Construct validity: The results of exploratory factor analysis
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.889, indicating that the sample was suitable for factor analysis. Bartlett’s test for sphericity was significant (Chi-square = 2666.587, DF = 120, p < 0.001), confirming the data were appropriate for structural identification. Exploratory factor analysis (EFA) was conducted using the maximum likelihood method and promax rotation. Four factors were extracted, which together explained 47.17% of the total variance in invisible violence. Seven items (Items 2, 7, 10, 13, 15, 20, and 21) did not load on any factor.
Factor 1: "Utilitarian-Benevolent sexist behavior"
This factor included items 8, 9, 11, 12, 22, and 23, explaining 13.76% of the total variance. Its eigenvalue was 2.203. The internal consistency of this factor, measured by Cronbach’s alpha and McDonald’s omega coefficients, was 0.803 and 0.806, respectively. The ICC for this factor was 0.859 (95% CI: 0.796–0.924). The highest mean scores were found for items 12 (2.66±1.54), 9 (2.19±1.41), 8 (2.18±1.42), and 11 (2.13±1.34).
Table 1. Sociodemographic information of married women who participated in the study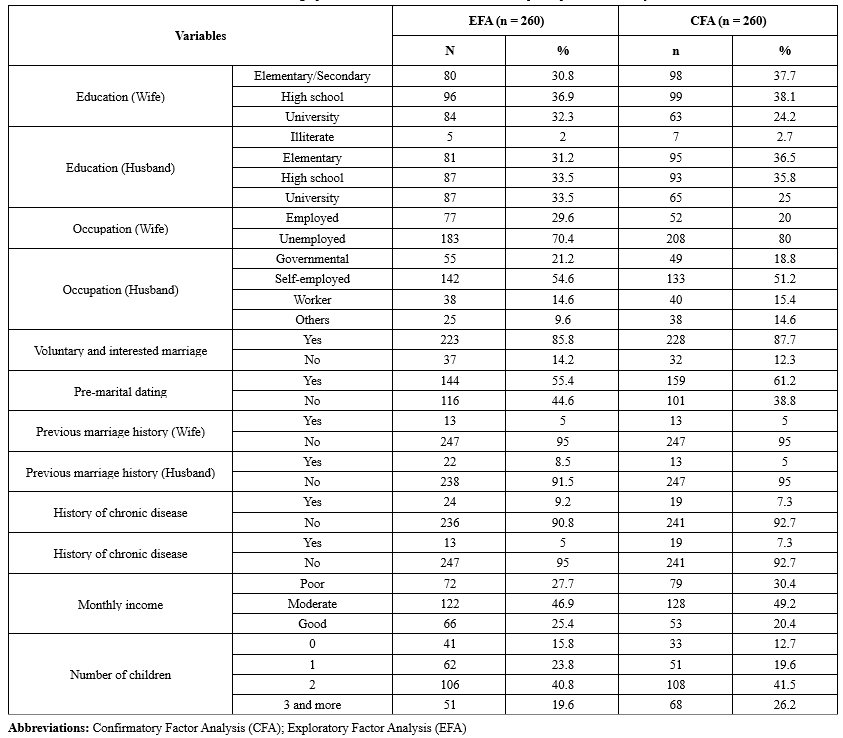 |
Factor 2: "Crisis sexist behavior"
This factor included items 3, 4, 5, and 6, explaining 12.1% of the total variance with an eigenvalue of 1.69. The internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.724 and 0.732, respectively. The ICC for this factor was 0.745 (95% CI: 0.579–0.862).
Factor 3: "Coercive sexist behavior"
This factor comprised items 1, 14, and 16. In the original version, items 13, 14, 15, and 16 were associated with coercive sexist behavior. However, in the Persian version, items 13 and 15 were removed, and item 1, which primarily indicated coercion, was included. Item 14 had the highest factor loading (0.726). This factor explained 12% of the total variance, with an eigenvalue of 1.67. Internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.733 and 0.736, respectively. The ICC for this factor was 0.911 (95% CI: 0.851–0.953).
Factor 4: "Ambivalent sexist behavior"
This factor included items 17, 18, and 19, explaining 9.3% of the total variance, with an eigenvalue of 1.30. The factor loadings for all three items were above 0.580. The internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.704 and 0.706, respectively. The lowest mean score was found for item 17 (1.32±0.82). The ICC for this factor was 0.832 (95% CI: 0.718-0.910) (Table 2).
Construct Validity: The results of CFA
The results of CFA on an additional 260 participants showed that the model extracted from the exploratory factor analysis fit well (Figure 1). The fit indices of the final model were as follows: CMIN = 205.434, DF = 96, CMIN/DF = 2.140, GFI = 0.952, AGFI = 0.932, NFI = 0.924, IFI = 0.958, CFI = 0.958, RMSEA = 0.047 (90% CI: 0.038–0.056).
This factor included items 3, 4, 5, and 6, explaining 12.1% of the total variance with an eigenvalue of 1.69. The internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.724 and 0.732, respectively. The ICC for this factor was 0.745 (95% CI: 0.579–0.862).
Factor 3: "Coercive sexist behavior"
This factor comprised items 1, 14, and 16. In the original version, items 13, 14, 15, and 16 were associated with coercive sexist behavior. However, in the Persian version, items 13 and 15 were removed, and item 1, which primarily indicated coercion, was included. Item 14 had the highest factor loading (0.726). This factor explained 12% of the total variance, with an eigenvalue of 1.67. Internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.733 and 0.736, respectively. The ICC for this factor was 0.911 (95% CI: 0.851–0.953).
Factor 4: "Ambivalent sexist behavior"
This factor included items 17, 18, and 19, explaining 9.3% of the total variance, with an eigenvalue of 1.30. The factor loadings for all three items were above 0.580. The internal consistency based on Cronbach’s alpha and McDonald’s omega was 0.704 and 0.706, respectively. The lowest mean score was found for item 17 (1.32±0.82). The ICC for this factor was 0.832 (95% CI: 0.718-0.910) (Table 2).
Construct Validity: The results of CFA
The results of CFA on an additional 260 participants showed that the model extracted from the exploratory factor analysis fit well (Figure 1). The fit indices of the final model were as follows: CMIN = 205.434, DF = 96, CMIN/DF = 2.140, GFI = 0.952, AGFI = 0.932, NFI = 0.924, IFI = 0.958, CFI = 0.958, RMSEA = 0.047 (90% CI: 0.038–0.056).
|
Table 2. The results of exploratory factor analysis of the Persian version of the Q-IVAW
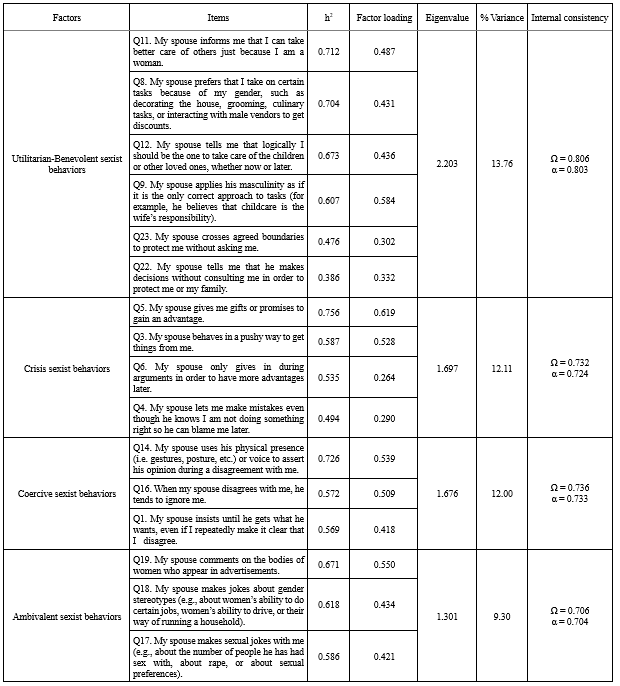 |
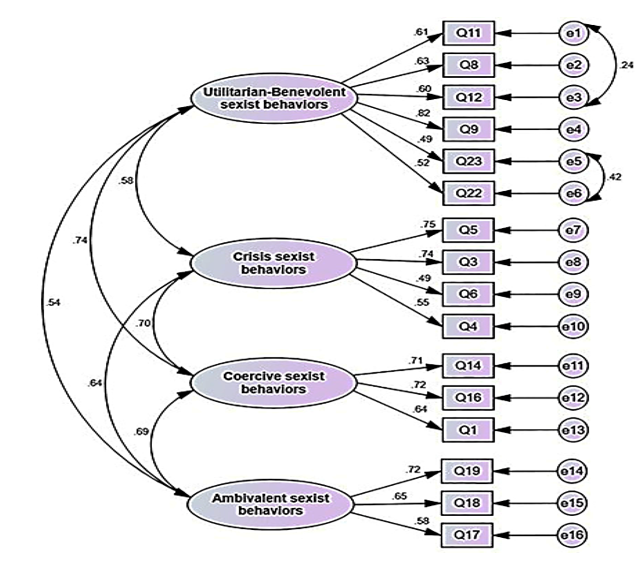 Figure 1. Path representation of the proposed four-factor model |
Discussion
The primary goal of this study was to evaluate the psychometric properties of the Persian version of the Q-IVAW, a tool designed to measure invisible violence against women. The results indicate that this version of the questionnaire is valid and reliable. Although the original version consists of five factors, the Persian version contains four.
The first factor in the Persian version includes items 8, 9, 11, 12, 22, and 23. In the original version, items 8 through 12 were associated with utilitarian sexist behaviors, while items 22 and 23 belonged to the benevolent sexist behaviors factor. We combined these items and labeled the factor “Utilitarian-Benevolent Sexist Behaviors” in the Persian version. Notably, item 10, which addresses the disregard for the economic value of women’s housework, was not assigned to any factor. The highest factor loading was associated with item 11, which refers to women being forced to care for others simply because they are women. The highest mean scores were found for the first four items, all of which relate to utilitarian-sexist behaviors. It seems that Iranian women have experienced the forms of invisible violence reflected in these items more than other forms. According to utilitarianism, actions that lead to happiness or pleasure are endorsed, while those that cause discomfort or harm are rejected (30). Benevolent sexism, a subtler form of sexism, is expressed positively but implicitly suggests women’s lack of competence (31,32). In some contexts, benevolent sexism manifests as a preference for men with benevolent sexist attitudes as romantic partners (33). Additionally, in countries with lower gender equality, the correlation between benevolent sexism and violence against women may be stronger than in more egalitarian countries due to stronger institutional support and punitive measures (34).
The second factor, labeled "Crisis Sexist Behaviors," includes items 3, 4, 5, and 6. In the original version, this factor consisted of 7 items (Items 1 to 7). However, in the Persian version, items 2 and 7 were not assigned to any factor, and item 1 was integrated into another factor. The highest factor loading in this factor was on item 5 (0.756), which refers to giving or promising something to gain a special advantage. The low mean score for items in this factor suggests that Iranian women have experienced these forms of invisible violence less frequently or may not recognize them as such. The third factor, labeled "Coercive Sexist Behavior," includes items 1, 14, and 16. In the Persian version, items 13 and 15 were omitted, as they were considered inconsistent with contemporary social norms in Iran, where women are active in the workforce. Item 1, originally assigned to "Critical Sexist Behavior" in the original version, was included in this factor, as it pertains to the enforcement of the husband’s orders, reflecting coercive control. The highest factor loading was observed for item 14 (0.726), which refers to a husband using physical stature and voice to impose his views. Coercive control is a form of ongoing abuse, involving intimidation, isolation, humiliation, surveillance, and exploitation to deprive individuals of their independence (35,36). If these methods fail, perpetrators may resort to physical and sexual violence (36).
The fourth factor, "Ambivalent Sexist Behavior," consisted of items 17 to 21 in the original version, but items 20 and 21 were not assigned to any factor in the Persian version. These items refer to “withholding information from a partner to avoid unnecessary conflict” and “feigning ignorance to justify harmful behavior.” The remaining three items were categorized as "Ambivalent Sexist Behavior," consistent with the original version. The highest factor loading in this factor was for item 19, which refers to men commenting on women’s appearance and physique in advertisements. The theory of ambivalent sexism posits that sexism manifests as hostility toward women who challenge traditional gender roles and male dominance, and it encompasses both benevolent and hostile sexism. Hostile sexism involves negative attitudes toward women, while benevolent sexism reflects positive attitudes toward traditional women, emphasizing the need to protect and support them (37,38).
This study found a relationship between the mean score of invisible violence and several variables, including the husband’s education and occupation, previous marriages, type of marriage (voluntary or arranged), premarital dating, and monthly income. The original study found that higher violence scores were associated with husbands with higher monthly incomes (23). This was explained by patriarchal norms, which suggest that men with greater financial resources exert more power in relationships (16). However, our study showed the opposite: the highest violence scores were associated with husbands with lower monthly incomes. This discrepancy may be due to the different demographic, cultural, and economic contexts in the two studies, as well as the severe economic challenges in Iran due to international sanctions. In the Persian version, the minimum and maximum mean scores were associated with items 17 and 12. The low mean score for item 17, about husbands making sexual jokes about their wives, may be due to the cultural sensitivity around extramarital affairs in Iran, which is considered a serious offense. This aligns with the findings of Adamczyk and Hayes (2012), who noted fewer extramarital affairs among married Hindus and Muslims compared to their Christian and Jewish counterparts (39). Item 12, which addresses a spouse telling the wife she should be the one to care for children and other loved ones, received the highest score. This reflects the patriarchal structure and gender roles in Iranian society, which allow male violence against women and encourage traditional gender roles (40). This study had several limitations. It focused only on literate women attending health centers in Asadabad, so caution should be taken when generalizing the results to all Iranian women. Additionally, few women visited the health centers with their husbands, which may have influenced their openness in answering questions. Therefore, women without their spouses were not asked to complete the questionnaires.
Conclusion
This methodological study shows that the Persian version of the questionnaire of invisible violence against women is a valid and reliable instrument that can be used to effectively assess this concept in the context of Iranian society. In traditional Iranian society, the term “violence against women” often evokes images of physical and sexual violence that can be proven and tracked based on the visible effects on a woman's body. Therefore, psychological violence is often overlooked. Invisible violence against women in traditional societies is frequently observed but often goes unnoticed because women’s rights are disregarded and they are unaware of these rights. The Persian version of the Q-IVAW, which has undergone psychometric evaluation, is able to measure this concept accurately. It can provide a clear understanding of the prevalence of invisible violence against Iranian women to inform officials, policymakers, researchers and society at large.
Acknowledgement
This study is derived from the research project No. 138, approved by the Ethics Committee of Asadabad School of Medical Sciences. The authors express their gratitude to the Scientific Council and Ethics Committee of Asadabad School of Medical Sciences, as well as to all the women who participated in this study.
Funding sources
This study was funded by the Asadabad School of Medical Sciences. The funding body had no role in the design of the study, data collection, interpretation of the result, or writing the manuscript.
Ethical statement
This study is the result of the project approved by the Asadabad School of Medical Sciences (IR.ASAUMS.REC.1402.028). According to the standards of Ethics in Research, the objectives of the study were explained to the research participants, and written informed consent was obtained to participate in the study. The questionnaires were distributed anonymously, and the participants were assured that their information would be kept confidential. All ethical principles in human research were observed in accordance with the Declaration of Helsinki.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
MR and RGG: manuscript preparation and study conceptualization; MR: data collection and manuscript preparation; RGG and FS: study design; RGG, AE, HSN, FS, and MR: writing-original draft preparation; RGG, AE, HSN, FS, and MR: writing-review and editing; AE and HSN: statistical analysis; RGG: project administration; MR: funding acquisition. All authors read and approved the finall version of the manuscript.
Data availability statement
All data on diagnostic yield analyzed in the current study are presented in the main text or supplementary material.
Type of study: Original Article |
Subject:
Midwifery
References
1. Bodaghabadi M. Prevalence of violence and related factors in pregnant women referring to Shahid Mobini hospital, Sabzevar. Hormozgan Medical Journal (HMJ). 2007;11(1):71-6. [View at Publisher] [Google Scholar]
2. Alijani F, Khosravi A, Mousavi MS, Delarosa V. The associated factors of domestic violence against infertile women. J Res Dev Nurs Midw. 2019;16(2):61-70. [View at Publisher] [DOI] [Google Scholar]
3. Knight M TD, Kenyon S, Shakespeare J, Gray R, Kurinczuk J, editors. Saving Lives, Improving Mothers' Care; Surveillance of maternal deaths in the UK 2011‐13 and lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009‐13. Oxford: National Perinatal Epidemiology Unit, University of Oxford; 2015. [View at Publisher] [Google Scholar]
4. Piquero AR, Jennings WG, Jemison E, Kaukinen C, Knaul FM. Domestic violence during the COVID-19 pandemic-Evidence from a systematic review and meta-analysis. J Crim Justice. 2021;74:101806. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Bifftu BB, Dachew BA, Tiruneh BT, Gezie LD, Guracho YD. Domestic violence related disclosure among women and girls in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2019;16(1):184. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Nakamura IB, Silva MT, Garcia LP, Galvao TF. Prevalence of physical violence against Brazilian women: systematic review and meta-analysis. Trauma Violence Abuse. 2023;24(2):329-39. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Hajnasiri H, Gheshlagh RG, Sayehmiri K, Moafi F, Farajzadeh M. Domestic violence among Iranian women: a systematic review and meta-analysis. Iran Red Crescent Med J. 2016;18(6):e34971. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Raziani Y, Hasheminasab L, Gheshlagh RG, Dalvand P, Baghi V, Aslani M. The prevalence of intimate partner violence among Iranian pregnant women: a systematic review and meta-analysis. Scand J Public Health. 2024;52(1):108-18. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Dey T, Thakar R. Domestic violence: an invisible pandemic. Obstet Gynaecol. 2022;24(2):90-2. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Trevillion K, Oram S, Feder G, Howard LM. Experiences of domestic violence and mental disorders: a systematic review and meta-analysis. PloS one. 2012;7(12):e51740. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Lee MS, Lee JJ, Lee H. Domestic Violence Experience, Past Depressive Disorder, Unplanned Pregnancy, and Suicide Risk in the First Year Postpartum: Mediating Effect of Postpartum Depression. Psychiatry Investig. 2024;21(10):1129-36. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Jackson EC, Renner LM, Flowers NI, Logeais ME, Clark CJ. Process evaluation of a systemic intervention to identify and support partner violence survivors in a multi-specialty health system. BMC Health Serv Res. 2020;20(1):996. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Van der Wath A. Women exposed to intimate partner violence: a Foucauldian discourse analysis of South African emergency nurses' perceptions. Afr Health Sci. 2019;19(2):1849-57. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Sönmez T, Apay SE, Taşgin A. The questionnaire for the detection of invisible violence against women. African Journal of Reproductive Health/La Revue Africaine de la Santé Reproductive. 2025;29(1):144-52. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Ayala A, Vives‐Cases C, Davó‐Blanes C, Rodríguez‐Blázquez C, Forjaz MJ, Bowes N, et al. Sexism and its associated factors among adolescents in Europe: Lights4Violence baseline results. Aggress Behav. 2021;47(3):354-63. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Bermúdez Figueroa E, Dabetić V, Yuste RP, Saeidzadeh Z. Gender and structural inequalities from a socio-legal perspective. InGender-competent legal education. Cham:Springer International Publishing;2023. p.95-142. [View at Publisher] [DOI] [Google Scholar]
17. Tlostanova M, Thapar-Björkert S, Koobak R. the postsocialist 'missing other'of transnational feminism? Feminist Review. 2019;121(1):81-7. [View at Publisher] [DOI] [Google Scholar]
18. Fernández-Antelo I, Cuadrado-Gordillo I, Martín-Mora Parra G. Synergy between acceptance of violence and sexist attitudes as a dating violence risk factor. Int J Environ Res Public Health. 2020;17(14):5209. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Martín-Fernández M, Gracia E, Lila M. A short measure of acceptability of intimate partner violence against women: development and validation of the A-IPVAW-8 scale. Assessment. 2022;29(5):896-908. [View at Publisher] [DOI] [PMID] [Google Scholar]
20. Ghanei Gheshlagh R, Barzanji A, Amini F, Zahednezhad H. Psychometric properties of the Farsi version of the Disaster Nursing Readiness Evaluation Index (F-DNREI). BMC Emerg Med. 2024;24(1):151. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Costello AB, Osborne J. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Practical assessment, research, and evaluation. 2019;10(1):7. [View at Publisher] [DOI] [Google Scholar]
22. Yu DS, Lee DT, Woo J. Issues and challenges of instrument translation. West J Nurs Res. 2004;26(3):307-20. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Dobarrio-Sanz I, Fernández-Vargas A, Fernández-Férez A, Vanegas-Coveña DP, Cordero-Ahiman OV, Granero-Molina J, et al. Development and psychometric assessment of a questionnaire for the detection of invisible violence against women. Int J Environ Res Public Health. 2022;19(17):11127. [View at Publisher] [DOI] [PMID] [Google Scholar]
24. Netemeyer RG BW, Sharma S. Scaling procedures: Issues and applications. sage publications;2003. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Baharuddin IH, Ismail N, Naing NN, Ibrahim K, Yasin SM, Patterson MS. Content and face validity of Workplace COVID-19 Knowledge & Stigma Scale (WoCKSS). BMC Public Health. 2024;24(1):874. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. DeVellis RF, Thorpe CT. Scale development: Theory and applications. Sage publications;2021. [View at Publisher] [Google Scholar]
27. Tavakol M, Wetzel A. Factor Analysis: a means for theory and instrument development in support of construct validity. Int J Med Educ. 2020;11:245. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Hu Lt, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal. 1999;6(1):1-55. [View at Publisher] [DOI] [Google Scholar]
29. Ebadi A Ausili D, Albatineh AN, Salarvand S, Ghanei Ghashlagh R. Psychometric evaluation of the Farsi version of the self-care of diabetes inventory in Iranian patients with diabetes. Diabetes Metab Syndr Obes. 2019;12:2775-84. [View at Publisher] [DOI] [PMID] [Google Scholar]
30. Vearrier L, Henderson CM, editors. Utilitarian principlism as a framework for crisis healthcare ethics. HEC forum. 2021;33(1-2):45-60. [View at Publisher] [DOI] [PMID] [Google Scholar]
31. Dardenne B, Dumont M, Bollier T. Insidious dangers of benevolent sexism: consequences for women's performance. J Pers Soc Psychol. 2007;93(5):764-79. [View at Publisher] [DOI] [PMID] [Google Scholar]
32. Mastari L, Spruyt B, Siongers J. Benevolent and hostile sexism in social spheres: The impact of parents, school and romance on Belgian adolescents' sexist attitudes.Front Sociol. 2019;4:47. [View at Publisher] [DOI] [PMID] [Google Scholar]
33. Lee TL, Fiske ST, Glick P, Chen Z. Ambivalent sexism in close relationships:(Hostile) power and (benevolent) romance shape relationship ideals. Sex Roles. 2010;62(7-8):583-601. [View at Publisher] [DOI] [PMID] [Google Scholar]
34. Corradi C, Stöckl H. The lessons of history: The role of the nation-states and the EU in fighting violence against women in 10 European countries. Current Sociology. 2016;64(4):671-88. [View at Publisher] [DOI] [Google Scholar]
35. Policastro C, Finn MA. Coercive control in intimate relationships: Differences across age and sex. J Interpers Violence. 2021;36(3-4):1520-43. [View at Publisher] [DOI] [PMID] [Google Scholar]
36. Loveland JE, Raghavan C. Coercive control, physical violence, and masculinity. Violence and Gender. 2017;4(1):5-10. [View at Publisher] [DOI] [Google Scholar]
37. Glick P, Lameiras M, Fiske ST, Eckes T, Masser B, Volpato C, et al. Bad but bold: Ambivalent attitudes toward men predict gender inequality in 16 nations. J Pers Soc Psychol. 2004;86(5):713-28. [View at Publisher] [DOI] [PMID] [Google Scholar]
38. Barreto M, Doyle DM. Benevolent and hostile sexism in a shifting global context. Nat Rev Psychol. 2023;2(2):98-111. [View at Publisher] [DOI] [PMID] [Google Scholar]
39. Adamczyk A, Hayes BE. Religion and sexual behaviors: Understanding the influence of Islamic cultures and religious affiliation for explaining sex outside of marriage. American sociological review. 2012;77(5):723-46. [View at Publisher] [DOI] [Google Scholar]
40. Ahmadi S, Hamidpoor K, Sedaghat H, Karami F. Violence against Women: The Rule of Patriarchal Ideology and the Hegemony of Male Domination (Case study: Women in Bushehr. Woman in Development and Politics. 2021;19(4):545-72. [View at Publisher] [DOI] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
