
Volume 21, Issue 2 (6-2024)
J Res Dev Nurs Midw 2024, 21(2): 11-15 |
Back to browse issues page


Ethics code: IR.SUMS.NUMIMG.REC.1401.064
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohebbi Z, Mohit M, Shirazi F, Ghaemmaghami P. The effect of damask rose aromatherapy on anxiety and pain in endoscopic lithotripsy patients: A Double-blind Randomized Clinical Trial. J Res Dev Nurs Midw 2024; 21 (2) :11-15
URL: http://nmj.goums.ac.ir/article-1-1634-en.html
URL: http://nmj.goums.ac.ir/article-1-1634-en.html



1- Nursing Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran
2- Surgical Technology Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran ,maryam.mohit71@gmail.com
3- School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran
2- Surgical Technology Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran ,
3- School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran
Full-Text [PDF 469 kb]
(1142 Downloads)
| Abstract (HTML) (2508 Views)
Full-Text: (1783 Views)
Introduction
Kidney stones represent a prevalent urological condition, necessitating treatment through a range of procedures, including transurethral lithotripsy (TUL), percutaneous nephrolithotomy (PCNL), and extracorporeal shock wave lithotripsy (ESWL). Presently, the aforementioned treatment modality has emerged as the primary therapeutic option for managing sizable kidney stones in the renal pelvic, Calix, and calyceal diverticulum (1).
In contemporary surgical practice, there has been a notable shift towards employing minimally invasive techniques in the treatment of patients across all medical disciplines. This trend is particularly pronounced in the realm of urological treatments pertaining to urinary system stones (2). The endoscopic approach has been shown to effectively decrease postoperative pain. This strategy has several advantages, including the reduction of hospitalization duration, cost reduction, and enhanced patient satisfaction. While endoscopic surgery has been shown to mitigate postoperative pain by minimizing tissue manipulation and utilizing smaller incisions, it is important to acknowledge that no surgical procedure is entirely devoid of pain and anxiety. Consequently, several approaches are employed to alleviate the pain and anxiety (3).
Surgery is commonly considered a stressful experience for both the patients and their family (4). Surgical anxiety has been found to induce alterations in the physiological functioning of the human body, hence posing potential risks to an individual's overall health and impeding the process of tissue recovery and repair (5). Anxiety has been seen to result in several physiological and behavioral manifestations. These include diminished appetite, discomfort, sleep disturbances, compromised immune function, delayed wound healing, elevated vital signs, impaired concentration, decreased engagement in self-care tasks, as well as lower collaboration with healthcare professionals (6).
The presence of anxiety has been found to impact the level of postoperative pain experienced and the subsequent healing process following anesthesia (7). Effective management of anxiety during the preoperative phase has the potential to promote cardiovascular stability, thus enhancing the patient's overall health throughout the surgical procedure and subsequent recovery period. Additionally, the management of anxiety has been found to be associated with a decrease in the use of anesthetics during surgical procedures, improved pain tolerance, and faster patient discharge from medical facilities (8).
Postoperative pain is among the most common and important issues of patient care. A significant majority of patients, over 80%, encounter immediate postoperative pain following surgical procedures, with about 70% of patients reporting pain levels ranging from moderate to severe (9,10). Recently, medication therapy is no longer regarded as the optimal and exclusive approach for mitigating the patients' pain and anxiety. While pharmaceuticals effectively alleviate the patient’s pain and anxiety, they frequently cause undesirable adverse reactions (11). In this context, the utilization of many approaches in supplementary medicine might prove advantageous. Complementary and alternative medicine (CAM) therapies encompass a range of strategies employed for disease prevention, treatment, and the enhancement of overall health and well-being in conjunction with conventional medical interventions. A widely embraced kind of alternative medicine that has gained significant popularity is aromatherapy, which involves the utilization of various aromatic substances (12, 13).
Damask rose is a medicinal plant whose essential oil is utilized in the practice of aromatherapy (14). It has been reported that rose has sedative, analgesic, antioxidant, antibacterial, and antidiabetic effects (15). Iran is recognized as one of the leading nations in rose production globally, which is well-known as Mohammadi flower, placing it in the top four countries in this industry (16). The purpose of this study is to investigate the potential benefits of aromatherapy, specifically the inhalation of Damask rose, on anxiety and pain experienced by patients undergoing endoscopic lithotripsy. Despite the increasing popularity of aromatherapy, there remains a limited number of studies that have examined its effectiveness in this context, highlighting the need for further investigation. Our research team aims to address this gap in the literature and provide valuable insights into the potential role of aromatherapy in improving patient outcomes in this population.
Methods
This study is a double-blind, randomized clinical trial that assessed the levels of pain and anxiety among patients both before and after the intervention in three distinct phases. The CONSORT flow chart of the randomized trial is shown in Figure 1. The research sample consisted of patients who were eligible for endoscopic lithotripsy, including TUL and PCNL, in hospitals affiliated with Shiraz University of Medical Sciences. These patients were recruited based on predetermined criteria using convenient sampling. To ensure randomization, a permutation block approach was employed to assign individuals to either the control or intervention group. Given that the participants were enrolled at two medical facilities, namely AliAsghar and Faqihi Hospitals, it was deemed appropriate to distribute the samples into ten blocks, each consisting of 6 samples, inside each respective facility. The process of random assignment to control and intervention groups was conducted using online web-based software.

Following the allocation of patients into the control and intervention groups, the Spielberger questionnaire and Visual Analog Scale (VAS) were completed prior to the implementation of the intervention in both groups. Subsequently, within the intervention group, the researcher applied a cotton pad infused with three drops of rose essential oil (40% concentration, Barich Company, Kashan) onto the patient's garments, securing it at a distance of 10 cm, using a plastic pin for a duration of 30 minutes. Subsequently, the patient was instructed to breathe normally. Following a period of 30 minutes, a colleague reassessed the patient's pain and anxiety levels (first stage).
The aromatherapy intervention was resumed by the researcher six hours after the operation and re-establishment of connection with the patients. All the measurements outlined in the initial stage were replicated for the patients enrolled in the intervention group. Subsequently, the colleague employed the aforementioned tools to assess the levels of pain and anxiety experienced by the patients following a 30-minute exposure to the rose aromatherapy (second stage).
In the control group, the researcher affixed a cotton material soaked in distilled water onto the patient's clothing using a plastic pin, positioning it at a distance of 10 cm for a duration of 30 minutes. Subsequently, a colleague assessed the level of pain and anxiety experienced by the participants (first stage). Six hours post-surgery, the researcher conducted a second round of measurements for the control group patients using the aforementioned tools. The questionnaires were administered by a colleague (second stage). All medical and nursing measures were taken similarly for both groups as the ward routine, and the research team measured the level of pain and anxiety at similar times in both groups.
The sample size was calculated based on the research conducted by Koohestani et al. (17). The significance level (α) was set at 0.05 and the power (β) at 0.20. Additionally, a confidence coefficient of 95% and a power of 80% were considered. Also, a 10% decrease in the number of participants was considered, resulting in a total of 60 individuals in each group.
The inclusion criteria in the study were effective communication skills, lack of dependence on drugs, absence of mental abnormalities, and avoidance from wearing perfume during the duration of the study. The exclusion criteria included respiratory and allergy conditions, patient noncompliance, and withdrawal from the study. The study objectives were presented to the patients by a trained research assistant. Additionally, the patients were instructed to complete the questionnaires. Participants had the autonomy to voluntarily discontinue their participation in the present study, ensuring the preservation of their rights and interests without any infringement. Subsequently, the patients were requested to provide written informed consent to voluntarily participate in the study. Furthermore, illiterate participants were provided informed consent by legal guardians. The research assistant collected the questionnaires when completed.
The data collection tools were three questionnaires: 1- demographic 2- visual analog scale (VAS) 3- Spielberger questionnaires. The VAS consists of horizontal lines ranging from 0 to 10, where 0 represents the absence of pain, and 10 represents the highest intensity of pain. The research assistant requested the participants to assess the magnitude of their pain using a standardized scale. The validity and reliability of the scale have been confirmed through several studies (18-20).
The Spielberger State-Trait Anxiety Inventory (STAI) questionnaire has several self-assessment measures designed to evaluate both overt and covert manifestations of anxiety. The overt anxiety scale comprises a set of 20 items designed to assess an individual's immediate and concurrent emotional state at the time of responding. The covert anxiety scale encompasses a set of 20 items designed to assess the individuals' overall and commonplace emotional states. The research conducted by Gustafson et al. (2020) employed Cronbach's alpha to assess the internal consistency of this tool, in which the obtained Cronbach's alpha coefficient of 0.93 suggests that the tool has proper internal consistency. Furthermore, the reliability of the tool, as measured by test-retest, was found to be 0.80, with a range of 0.66 to 0.89 (21).
Descriptive statistics were employed to summarize the data, while independent t-tests were used to examine the differences between the groups. Repeated measures analysis of variance was utilized to assess the effects of multiple measurements, followed by Bonferroni post- hoc testing and marginal effect for pairwise comparisons. The collected data were analyzed using SPSS 21 software.
Results
A total of 120 patients participated in this study, with a majority being male (61.7%). Among the participants, 35 individuals (29.2%) possessed either a diploma or a bachelor's degree. The mean age, height, and weight of the subjects were 47.79±14.48 years, 166.88±8.80 cm, and 70.83±12.19 kg, respectively. The statistical analyses revealed no statistically significant differences between the two groups regarding their demographic characteristics (Table 1).
The repeated measure analysis of variance revealed a statistically significant effect of time on the mean pain levels (P < 0.001). Hence, owing to the importance of the interaction, marginal averages (also known as marginal effects) were employed for both intra-group and inter-group comparisons in all instances (Table 2).
Regarding the pain variable, the results indicated that prior to the intervention, there were no statistically significant differences in the mean pain levels between the two groups (P=0.489). During the initial phase of the intervention, the intervention group exhibited a statistically significant reduction in the mean pain by 2.20 units compared to the control group (P < 0.001). Furthermore, following the surgical procedure and throughout the second phase of the intervention, it was seen that the pain in the intervention group was 5.03 units lower compared to the control group (P < 0.001). Furthermore, the mean difference between various time within the control and intervention groups was presented in Table 3.
About the analysis of overt anxiety, the utilization of marginal averages was necessary for both intra-group and inter-group comparisons in all instances, owing to the observed significance of the interaction effect (P=0.04). The mean difference of this measure between the intervention and control groups prior to the intervention was 0.17. However, this difference was not statistically significant (P=0.862). During the initial stage of the intervention, the mean anxiety level in the intervention group was found to be 2.47 units lower than that of the control group (P=0.021). Furthermore, during the second stage of the intervention, the mean anxiety level in the intervention group showed a reduction of 2.02 units compared to the control group (P < 0.001). Moreover, the mean difference overt anxiety between various time within the control and intervention groups was presented in Table 4.
To facilitate the comparison of covert anxiety, the marginal mean was employed for both intra-group and inter-group comparisons in all instances, given the significance of the interaction effect (P=0.013). Regarding the covert anxiety variable, the results indicated that prior to the intervention, there were no statistically significant differences (P=0.868) in the mean covert anxiety levels between the two groups, suggesting that the two groups were comparable in terms of this variable. During the initial stage of the intervention, the intervention group exhibited a statistically significant reduction of 3.55 units in covert anxiety compared to the control group (P=0.003). Furthermore, during the second stage of the intervention, the mean level of covert anxiety exhibited a reduction of 2.13 units in the intervention group compared with the control group (P < 0.001). In addition, the mean difference covert anxiety between various time within the control and intervention groups was presented in Table 5.
Discussion
The present study was conducted to examine the impact of rose aromatherapy on the levels of anxiety and pain experienced by patients undergoing endoscopic lithotripsy. The findings of this study indicated that within the intervention group, the damask rose aromatherapy resulted in a significant reduction in the mean pain throughout the initial and second phases of the intervention, as compared to the baseline period. Furthermore, the results of the present study indicated that the intervention group experienced a reduction in the mean levels of overt and covert anxieties during both stages of aromatherapy, as compared to the control group.
Sadeghi et al. (2020) conducted a study to investigate the impact of damask rose aromatherapy on the level of pain experienced by burn patients. The findings of their study revealed a significant reduction in pain intensity among patients following the intervention (18). A meta-analysis conducted by Nasiri et al. (2021) examined the impact of damask rose aromatherapy on the severity of acute pain in adults. The study revealed a significant decrease in pain intensity among patients following the intervention (22). The study conducted by Bastani and colleagues in 2017 demonstrated that using damask rose essence in aromatherapy can have a positive impact on pain relief following knee arthroscopic surgery (23). Additionally, a study by Roozbahani and team in 2015 found that inhalation of damask rose water can help reduce labor pain (p < 0.001), which supports the findings of the current study (24).
A clinical trial by Abbasi et al. (2020) examined the impact of damask rose aromatherapy on the severity of postoperative pain, the overt and covert anxiety levels experienced by women after a caesarean section. The researchers employed damask rose essential oil as an intervention for a duration of 30 minutes among the participants. The researchers demonstrated a significant reduction in maternal pain levels, and also the mean score of overt and covert anxiety following surgery was significantly lower in the intervention group compared to the control group (4), which supports the findings of the current study. Moreover, in line with the present study, Bikmoradi et al. examined the impact of damask rose aromatherapy on anxiety levels among patients undergoing coronary angiography. The study demonstrated a statistically significant difference in the mean anxiety score in the intervention group compared with the control group (25).
Farzaneh et al. (2022) investigated the impact of damask rose aromatherapy on the levels of overt and covert anxiety among patients scheduled for lithotripsy operations prior to the procedure. A statistically significant difference (P < 0.001) was seen when they compared the mean levels of overt and covert anxiety between the control and intervention groups. They revealed a reduction in overt and covert anxiety levels among patients in the intervention group prior to surgery (26). Also, Mirzaee et al. conducted a study that demonstrated the effectiveness of Damask rose essential oil aromatherapy in reducing pre-endoscopic anxiety among patients (27).
Fazlollahpour et al.'s study aimed to examine the impact of inhaling rose essential oil through aromatherapy on anxiety levels in patients undergoing coronary artery bypass graft. The findings of this study indicated that, in contrast to the current study, there was no significant reduction in the severity of anxiety observed among the intervention groups (28). This lack of significant effect may potentially be attributed to the duration of exposure to the rose aroma. Azizi et al. (2018) conducted a study that demonstrated a reduction in pain before and after dressing through the inhalation of lavender essence. Furthermore, there was no meaningful variance in pain intensity between the placebo and control groups. The primary distinction between the current study and the earlier one is the inhaler type used (29). The research conducted in this study was focused on patients who underwent lithotripsy procedures. The study has several limitations, including the reluctance of some patients to cooperate in the research, the absence of a dedicated space for implementing aromatherapy, and the lack of comparable studies on damask rose inhalation in this patient population. Consequently, it was not feasible to draw comparisons with existing research findings. As a result, prospective studies should focus on replicating this research with a different demographic and patients with varied medical conditions, exploring diverse aromas, and investigating the optimal duration of aromatherapy.
Conclusion
The use of inhalation damask rose aromatherapy was found to result in temporary pain alleviation and a decrease in both overt and covert anxiety levels among individuals following endoscopic lithotripsy. Given the cost-effectiveness of this intervention for patients, nurses can employ it as a kind of individualized treatment to attain relaxation and secure its short-term advantages.
Acknowledgement
This project resulted from an MSc thesis in Surgical Technology Major at Shiraz University of Medical Sciences. The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran and also the Center for Development of Clinical Research of Nemazee Hospital and Dr Nasrin Shokrpour for editorial assistance.
Funding sources
This research was supported by Shiraz University of Medical Sciences (Grant No. 26218).
Ethical statement
The current study was approved by the research ethics committee of Shiraz University of Medical Sciences (IR.SUMS.NUMIMG.REC.1401.064). Additionally, it has been registered in the Iranian Registry of Clinical Trials (IRCT) with the registration code of IRCT20100919004775N14.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
All authors participated in the conception and design of the study. MM and ZM contributed to proposal preparation and data collection. MM and PGH participated in data analysis and interpretation. MM, FSH and ZM contributed to drafting of the article. All authors have seen and approved the submitted version of this manuscript.
Kidney stones represent a prevalent urological condition, necessitating treatment through a range of procedures, including transurethral lithotripsy (TUL), percutaneous nephrolithotomy (PCNL), and extracorporeal shock wave lithotripsy (ESWL). Presently, the aforementioned treatment modality has emerged as the primary therapeutic option for managing sizable kidney stones in the renal pelvic, Calix, and calyceal diverticulum (1).
In contemporary surgical practice, there has been a notable shift towards employing minimally invasive techniques in the treatment of patients across all medical disciplines. This trend is particularly pronounced in the realm of urological treatments pertaining to urinary system stones (2). The endoscopic approach has been shown to effectively decrease postoperative pain. This strategy has several advantages, including the reduction of hospitalization duration, cost reduction, and enhanced patient satisfaction. While endoscopic surgery has been shown to mitigate postoperative pain by minimizing tissue manipulation and utilizing smaller incisions, it is important to acknowledge that no surgical procedure is entirely devoid of pain and anxiety. Consequently, several approaches are employed to alleviate the pain and anxiety (3).
Surgery is commonly considered a stressful experience for both the patients and their family (4). Surgical anxiety has been found to induce alterations in the physiological functioning of the human body, hence posing potential risks to an individual's overall health and impeding the process of tissue recovery and repair (5). Anxiety has been seen to result in several physiological and behavioral manifestations. These include diminished appetite, discomfort, sleep disturbances, compromised immune function, delayed wound healing, elevated vital signs, impaired concentration, decreased engagement in self-care tasks, as well as lower collaboration with healthcare professionals (6).
The presence of anxiety has been found to impact the level of postoperative pain experienced and the subsequent healing process following anesthesia (7). Effective management of anxiety during the preoperative phase has the potential to promote cardiovascular stability, thus enhancing the patient's overall health throughout the surgical procedure and subsequent recovery period. Additionally, the management of anxiety has been found to be associated with a decrease in the use of anesthetics during surgical procedures, improved pain tolerance, and faster patient discharge from medical facilities (8).
Postoperative pain is among the most common and important issues of patient care. A significant majority of patients, over 80%, encounter immediate postoperative pain following surgical procedures, with about 70% of patients reporting pain levels ranging from moderate to severe (9,10). Recently, medication therapy is no longer regarded as the optimal and exclusive approach for mitigating the patients' pain and anxiety. While pharmaceuticals effectively alleviate the patient’s pain and anxiety, they frequently cause undesirable adverse reactions (11). In this context, the utilization of many approaches in supplementary medicine might prove advantageous. Complementary and alternative medicine (CAM) therapies encompass a range of strategies employed for disease prevention, treatment, and the enhancement of overall health and well-being in conjunction with conventional medical interventions. A widely embraced kind of alternative medicine that has gained significant popularity is aromatherapy, which involves the utilization of various aromatic substances (12, 13).
Damask rose is a medicinal plant whose essential oil is utilized in the practice of aromatherapy (14). It has been reported that rose has sedative, analgesic, antioxidant, antibacterial, and antidiabetic effects (15). Iran is recognized as one of the leading nations in rose production globally, which is well-known as Mohammadi flower, placing it in the top four countries in this industry (16). The purpose of this study is to investigate the potential benefits of aromatherapy, specifically the inhalation of Damask rose, on anxiety and pain experienced by patients undergoing endoscopic lithotripsy. Despite the increasing popularity of aromatherapy, there remains a limited number of studies that have examined its effectiveness in this context, highlighting the need for further investigation. Our research team aims to address this gap in the literature and provide valuable insights into the potential role of aromatherapy in improving patient outcomes in this population.
Methods
This study is a double-blind, randomized clinical trial that assessed the levels of pain and anxiety among patients both before and after the intervention in three distinct phases. The CONSORT flow chart of the randomized trial is shown in Figure 1. The research sample consisted of patients who were eligible for endoscopic lithotripsy, including TUL and PCNL, in hospitals affiliated with Shiraz University of Medical Sciences. These patients were recruited based on predetermined criteria using convenient sampling. To ensure randomization, a permutation block approach was employed to assign individuals to either the control or intervention group. Given that the participants were enrolled at two medical facilities, namely AliAsghar and Faqihi Hospitals, it was deemed appropriate to distribute the samples into ten blocks, each consisting of 6 samples, inside each respective facility. The process of random assignment to control and intervention groups was conducted using online web-based software.
Following the allocation of patients into the control and intervention groups, the Spielberger questionnaire and Visual Analog Scale (VAS) were completed prior to the implementation of the intervention in both groups. Subsequently, within the intervention group, the researcher applied a cotton pad infused with three drops of rose essential oil (40% concentration, Barich Company, Kashan) onto the patient's garments, securing it at a distance of 10 cm, using a plastic pin for a duration of 30 minutes. Subsequently, the patient was instructed to breathe normally. Following a period of 30 minutes, a colleague reassessed the patient's pain and anxiety levels (first stage).
The aromatherapy intervention was resumed by the researcher six hours after the operation and re-establishment of connection with the patients. All the measurements outlined in the initial stage were replicated for the patients enrolled in the intervention group. Subsequently, the colleague employed the aforementioned tools to assess the levels of pain and anxiety experienced by the patients following a 30-minute exposure to the rose aromatherapy (second stage).
In the control group, the researcher affixed a cotton material soaked in distilled water onto the patient's clothing using a plastic pin, positioning it at a distance of 10 cm for a duration of 30 minutes. Subsequently, a colleague assessed the level of pain and anxiety experienced by the participants (first stage). Six hours post-surgery, the researcher conducted a second round of measurements for the control group patients using the aforementioned tools. The questionnaires were administered by a colleague (second stage). All medical and nursing measures were taken similarly for both groups as the ward routine, and the research team measured the level of pain and anxiety at similar times in both groups.
The sample size was calculated based on the research conducted by Koohestani et al. (17). The significance level (α) was set at 0.05 and the power (β) at 0.20. Additionally, a confidence coefficient of 95% and a power of 80% were considered. Also, a 10% decrease in the number of participants was considered, resulting in a total of 60 individuals in each group.
The inclusion criteria in the study were effective communication skills, lack of dependence on drugs, absence of mental abnormalities, and avoidance from wearing perfume during the duration of the study. The exclusion criteria included respiratory and allergy conditions, patient noncompliance, and withdrawal from the study. The study objectives were presented to the patients by a trained research assistant. Additionally, the patients were instructed to complete the questionnaires. Participants had the autonomy to voluntarily discontinue their participation in the present study, ensuring the preservation of their rights and interests without any infringement. Subsequently, the patients were requested to provide written informed consent to voluntarily participate in the study. Furthermore, illiterate participants were provided informed consent by legal guardians. The research assistant collected the questionnaires when completed.
The data collection tools were three questionnaires: 1- demographic 2- visual analog scale (VAS) 3- Spielberger questionnaires. The VAS consists of horizontal lines ranging from 0 to 10, where 0 represents the absence of pain, and 10 represents the highest intensity of pain. The research assistant requested the participants to assess the magnitude of their pain using a standardized scale. The validity and reliability of the scale have been confirmed through several studies (18-20).
The Spielberger State-Trait Anxiety Inventory (STAI) questionnaire has several self-assessment measures designed to evaluate both overt and covert manifestations of anxiety. The overt anxiety scale comprises a set of 20 items designed to assess an individual's immediate and concurrent emotional state at the time of responding. The covert anxiety scale encompasses a set of 20 items designed to assess the individuals' overall and commonplace emotional states. The research conducted by Gustafson et al. (2020) employed Cronbach's alpha to assess the internal consistency of this tool, in which the obtained Cronbach's alpha coefficient of 0.93 suggests that the tool has proper internal consistency. Furthermore, the reliability of the tool, as measured by test-retest, was found to be 0.80, with a range of 0.66 to 0.89 (21).
Descriptive statistics were employed to summarize the data, while independent t-tests were used to examine the differences between the groups. Repeated measures analysis of variance was utilized to assess the effects of multiple measurements, followed by Bonferroni post- hoc testing and marginal effect for pairwise comparisons. The collected data were analyzed using SPSS 21 software.
Results
A total of 120 patients participated in this study, with a majority being male (61.7%). Among the participants, 35 individuals (29.2%) possessed either a diploma or a bachelor's degree. The mean age, height, and weight of the subjects were 47.79±14.48 years, 166.88±8.80 cm, and 70.83±12.19 kg, respectively. The statistical analyses revealed no statistically significant differences between the two groups regarding their demographic characteristics (Table 1).
Table 1. Participants’ demographics of intervention and control groups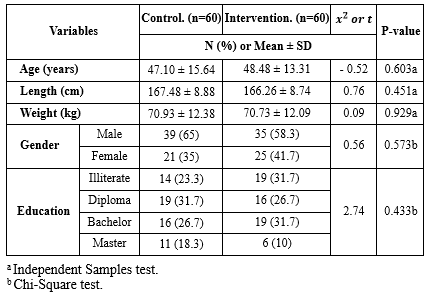 |
Table 2. Evaluating repeated measurements variance for intergroup and intragroup effects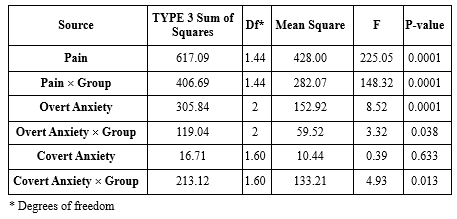 |
About the analysis of overt anxiety, the utilization of marginal averages was necessary for both intra-group and inter-group comparisons in all instances, owing to the observed significance of the interaction effect (P=0.04). The mean difference of this measure between the intervention and control groups prior to the intervention was 0.17. However, this difference was not statistically significant (P=0.862). During the initial stage of the intervention, the mean anxiety level in the intervention group was found to be 2.47 units lower than that of the control group (P=0.021). Furthermore, during the second stage of the intervention, the mean anxiety level in the intervention group showed a reduction of 2.02 units compared to the control group (P < 0.001). Moreover, the mean difference overt anxiety between various time within the control and intervention groups was presented in Table 4.
To facilitate the comparison of covert anxiety, the marginal mean was employed for both intra-group and inter-group comparisons in all instances, given the significance of the interaction effect (P=0.013). Regarding the covert anxiety variable, the results indicated that prior to the intervention, there were no statistically significant differences (P=0.868) in the mean covert anxiety levels between the two groups, suggesting that the two groups were comparable in terms of this variable. During the initial stage of the intervention, the intervention group exhibited a statistically significant reduction of 3.55 units in covert anxiety compared to the control group (P=0.003). Furthermore, during the second stage of the intervention, the mean level of covert anxiety exhibited a reduction of 2.13 units in the intervention group compared with the control group (P < 0.001). In addition, the mean difference covert anxiety between various time within the control and intervention groups was presented in Table 5.
|
Table 3. Multiple comparisons of means of pain intensity before and after intervention in two groups using Bonferroni test
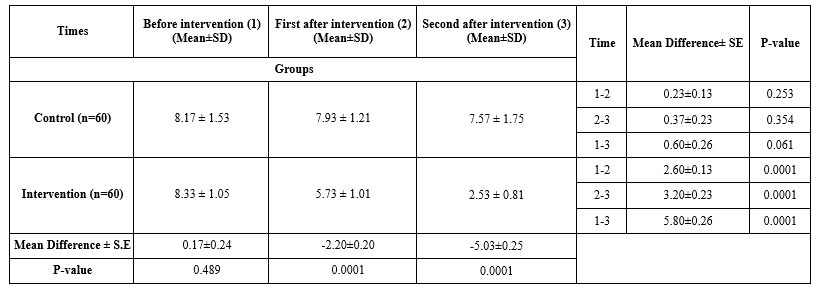 Table 4. Multiple comparisons of means of Overt Anxiety before and after intervention in two groups using Bonferroni test 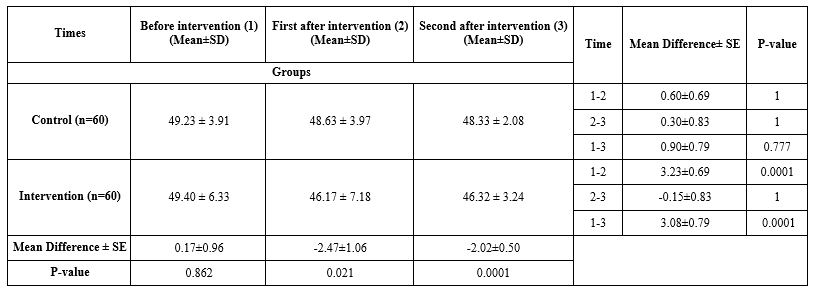 Table 5. Multiple comparisons of means of Covert Anxiety before and after intervention in two groups using Bonferroni test  |
Discussion
The present study was conducted to examine the impact of rose aromatherapy on the levels of anxiety and pain experienced by patients undergoing endoscopic lithotripsy. The findings of this study indicated that within the intervention group, the damask rose aromatherapy resulted in a significant reduction in the mean pain throughout the initial and second phases of the intervention, as compared to the baseline period. Furthermore, the results of the present study indicated that the intervention group experienced a reduction in the mean levels of overt and covert anxieties during both stages of aromatherapy, as compared to the control group.
Sadeghi et al. (2020) conducted a study to investigate the impact of damask rose aromatherapy on the level of pain experienced by burn patients. The findings of their study revealed a significant reduction in pain intensity among patients following the intervention (18). A meta-analysis conducted by Nasiri et al. (2021) examined the impact of damask rose aromatherapy on the severity of acute pain in adults. The study revealed a significant decrease in pain intensity among patients following the intervention (22). The study conducted by Bastani and colleagues in 2017 demonstrated that using damask rose essence in aromatherapy can have a positive impact on pain relief following knee arthroscopic surgery (23). Additionally, a study by Roozbahani and team in 2015 found that inhalation of damask rose water can help reduce labor pain (p < 0.001), which supports the findings of the current study (24).
A clinical trial by Abbasi et al. (2020) examined the impact of damask rose aromatherapy on the severity of postoperative pain, the overt and covert anxiety levels experienced by women after a caesarean section. The researchers employed damask rose essential oil as an intervention for a duration of 30 minutes among the participants. The researchers demonstrated a significant reduction in maternal pain levels, and also the mean score of overt and covert anxiety following surgery was significantly lower in the intervention group compared to the control group (4), which supports the findings of the current study. Moreover, in line with the present study, Bikmoradi et al. examined the impact of damask rose aromatherapy on anxiety levels among patients undergoing coronary angiography. The study demonstrated a statistically significant difference in the mean anxiety score in the intervention group compared with the control group (25).
Farzaneh et al. (2022) investigated the impact of damask rose aromatherapy on the levels of overt and covert anxiety among patients scheduled for lithotripsy operations prior to the procedure. A statistically significant difference (P < 0.001) was seen when they compared the mean levels of overt and covert anxiety between the control and intervention groups. They revealed a reduction in overt and covert anxiety levels among patients in the intervention group prior to surgery (26). Also, Mirzaee et al. conducted a study that demonstrated the effectiveness of Damask rose essential oil aromatherapy in reducing pre-endoscopic anxiety among patients (27).
Fazlollahpour et al.'s study aimed to examine the impact of inhaling rose essential oil through aromatherapy on anxiety levels in patients undergoing coronary artery bypass graft. The findings of this study indicated that, in contrast to the current study, there was no significant reduction in the severity of anxiety observed among the intervention groups (28). This lack of significant effect may potentially be attributed to the duration of exposure to the rose aroma. Azizi et al. (2018) conducted a study that demonstrated a reduction in pain before and after dressing through the inhalation of lavender essence. Furthermore, there was no meaningful variance in pain intensity between the placebo and control groups. The primary distinction between the current study and the earlier one is the inhaler type used (29). The research conducted in this study was focused on patients who underwent lithotripsy procedures. The study has several limitations, including the reluctance of some patients to cooperate in the research, the absence of a dedicated space for implementing aromatherapy, and the lack of comparable studies on damask rose inhalation in this patient population. Consequently, it was not feasible to draw comparisons with existing research findings. As a result, prospective studies should focus on replicating this research with a different demographic and patients with varied medical conditions, exploring diverse aromas, and investigating the optimal duration of aromatherapy.
Conclusion
The use of inhalation damask rose aromatherapy was found to result in temporary pain alleviation and a decrease in both overt and covert anxiety levels among individuals following endoscopic lithotripsy. Given the cost-effectiveness of this intervention for patients, nurses can employ it as a kind of individualized treatment to attain relaxation and secure its short-term advantages.
Acknowledgement
This project resulted from an MSc thesis in Surgical Technology Major at Shiraz University of Medical Sciences. The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran and also the Center for Development of Clinical Research of Nemazee Hospital and Dr Nasrin Shokrpour for editorial assistance.
Funding sources
This research was supported by Shiraz University of Medical Sciences (Grant No. 26218).
Ethical statement
The current study was approved by the research ethics committee of Shiraz University of Medical Sciences (IR.SUMS.NUMIMG.REC.1401.064). Additionally, it has been registered in the Iranian Registry of Clinical Trials (IRCT) with the registration code of IRCT20100919004775N14.
Conflicts of interest
The authors declare that they have no competing interests.
Author contributions
All authors participated in the conception and design of the study. MM and ZM contributed to proposal preparation and data collection. MM and PGH participated in data analysis and interpretation. MM, FSH and ZM contributed to drafting of the article. All authors have seen and approved the submitted version of this manuscript.
Type of study: Original Article |
Subject:
Nursing
References
1. Baralo B, Samson P, Hoenig D, Smith A. Percutaneous kidney stone surgery and radiation exposure: A review. Asian J Urol. 2020;7(1):10-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Hernandez N, Mozafarpour S, Song Y, Eisner BH. Cessation of ureteral colic does not necessarily mean that a ureteral stone has been expelled. J Urol. 2018;199(4):1011-4. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Noh GO, Park KS. Effects of aroma self-foot reflexology on peripheral neuropathy, peripheral skin temperature, anxiety, and depression in gynaecologic cancer patients undergoing chemotherapy: A randomised controlled trial. Eur J Oncol Nurs. 2019;42:82-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Abbasijahromi A, Hojati H, Nikooei S, Jahromi HK, Dowlatkhah HR, Zarean V, et al. Compare the effect of aromatherapy using lavender and Damask rose essential oils on the level of anxiety and severity of pain following C-section: A double-blinded randomized clinical trial. J Complement Integr Med. 2020;17(3). [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Rahmati H, Seidi J, Ghodsbin F, Rahımı S, Gholamvaısı B. The effect of music therapy on anxiety in patients before elective general surgery. International Journal of Pharmaceutical Research. 2018;10(3):136-42. [View at Publisher] [DOI] [Google Scholar]
6. Ghimire R, Poudel P. Preoperative anxiety and its determinants among patients scheduled for major surgery: a hospital based study. J Anesthesiol. 2018;6(2):57-60. [View at Publisher] [Google Scholar]
7. Renaud-Roy E, Stöckle P-A, Maximos S, Brulotte V, Sideris L, Dubé P, et al. Correlation between incremental remifentanil doses and the Nociception Level (NOL) index response after intraoperative noxious stimuli. Can J Anesth. 2019;66(9):1049-61. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Shirzad M, Nasiri E, Hesamirostami MH, Akbari H. Comparing the effects of rose essential oil and Benson relaxation technique on preoperative anxiety and hemodynamic status and postoperative complications in rhinoplasty candidates. Complementary Medicine Journal. 2021;11(2):180-91. [View at Publisher] [DOI] [Google Scholar]
9. Vatankhah M, Melekshoar M. Comparison of the prophylactic effect of ibuprofen and intravenous ketorolac in pain control after upper extremity surgery: A Double-Blind Randomized Clinical Trial Study. medical journal of mashhad university of medical sciences. 2021;64(2):2692-705. [View at Publisher] [DOI] [Google Scholar]
10. Lin CL, Hwang SL, Jiang P, Hsiung NH. Effect of music therapy on pain after orthopedic surgery-a systematic review and meta‐analysis. Pain Practice. 2020;20(4):422-36. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Babatabar Darzi H, Vahedian‐Azimi A, Ghasemi S, Ebadi A, Sathyapalan T, Sahebkar A. The effect of aromatherapy with rose and lavender on anxiety, surgical site pain, and extubation time after open‐heart surgery: A double‐center randomized controlled trial. Phytother Res. 2020;34(10):2675-84. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Grossman LD, Roscoe R, Shack AR, Committee DCCPGE. Complementary and alternative medicine for diabetes. Can J Diabetes. 2018;42(Suppl1):S154-61. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Farzaneh M, Abbasijahromi A, Saadatmand V, Parandavar N, Dowlatkhah HR, Bahmanjahromi A. Comparative effect of nature-based sounds intervention and headphones intervention on pain severity after cesarean section: a prospective double-blind randomized trial. Anesth Pain Med. 2019;9(2):e67835. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Kheirkhah M, Valipour NS, Neisani Samani L, Haghani H. Effect of aromatherapy with essential damask rose oil on anxiety of the active phase of labor nulliparous women. Nursing and Midwifery Journal (UMSU). 2013;11(6). [View at Publisher] [Google Scholar]
15. Hamdamian S, Nazarpour S, Simbar M, Hajian S, Mojab F, Talebi A. Effects of aromatherapy with Rosa damascena on nulliparous women's pain and anxiety of labor during first stage of labor. J Integr Med. 2018;16(2):120-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Boskabady MH, Shafei MN, Saberi Z, Amini S. Pharmacological effects of Rosa damascena. Iran J Basic Med Sci. 2011;14(4):295-307. [View at Publisher] [PMID] [Google Scholar]
17. Koohestani Ein-O-Din R, Faghih A, Ahmadi Z, Jamhiri R, Hosseini Teshnizi S, Farshidi H. The effect of inhalation of peppermint aroma on anxiety in patients undergoing coronary angiography. Hayat. 2020;26(3):266-79. [View at Publisher] [Google Scholar]
18. Sadeghi N, Azizi A, Asgari S, Mohammadi Y. The effect of inhalation aromatherapy with damask rose essence on pain intensity and anxiety in burned patients: A single-blind randomized clinical trial. Burns. 2020;46(8):1933-41. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Begum MR, Hossain MA. Validity and reliability of visual analogue scale (VAS) for pain measurement. Journal of Medical Case Reports and Reviews. 2019;2(11):394-402. [View at Publisher] [Google Scholar]
20. Delgado DA, Lambert BS, Boutris N, McCulloch PC, Robbins AB, Moreno MR, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Gustafson L, Gabel P, Hammer A, Lauridsen H, Petersen L, Andersen B, et al. Validity and reliability of State-Trait Anxiety Inventory in Danish women aged 45 years and older with abnormal cervical screening results. BMC Med Res Methodol. 2020;20(1):89. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Nasiri M, Torkaman M, Feizi S, Shamloo MBB. Effect of aromatherapy with Damask rose on alleviating adults' acute pain severity: A systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. 2021;56:102596. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Bastani F, Kia PS, Haghani H. Effect of aromatherapy with Damask Rose (Rosa damascena Mill.) on anxiety in the elderly: Open-labeled quasi-experimental placebo-controlled trial. Iran J Psychiatry Behav Sci. 2020;14(4):e58064. [View at Publisher] [DOI] [Google Scholar]
24. Roozbahani N, Attarha M, Akbari Torkestani N, Amiri Farahani L, Heidari T. The effect of rose water aromatherapy on reducing labor pain in primiparous women. Complementary Medicine Journal. 2015;5(1):1042-53. [View at Publisher] [Google Scholar]
25. Bikmoradi A, Roshanaei G, Moradkhani S, Fatahi A. Impact of inhalation aromatherapy with damask rose on anxiety of patients undergoing coronary angiography: A single-blind randomized controlled clinical trial. Avicenna J Nurs Midwifery Care. 2020;28(2):93-102. [View at Publisher] [DOI] [Google Scholar]
26. Farzaneh M, Zarean V, Abbasijahromi A, Mohit M, Amirkhani M, Badiyepeymaiejahromi Z, et al. A randomized controlled trial examining the effect of aromatherapy using the damask rose essential oil on pre-operative anxiety levels. Nephro-Urology Monthly. 2022;14(2):e116696. [View at Publisher] [DOI] [Google Scholar]
27. Mirzaee Jirdehi M, Monfared A, Mansour Ghanaei F, Kazemnezhad Leili E. Damask rose aromatherapy and the anxiety of endoscopic candidate patients: A clinical trial. Journal of Holistic Nursing and Midwifery. 2021;31(3):203-11. [View at Publisher] [DOI] [Google Scholar]
28. Fazlollahpour-Rokni F, Shorofi SA, Mousavinasab N, Ghafari R, Esmaeili R. The effect of inhalation aromatherapy with rose essential oil on the anxiety of patients undergoing coronary artery bypass graft surgery. Complement Ther Clin Pract. 2019;34:201-7. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Azizi A, Oshvandi K, Farhahian M, Lashani A. The effect of inhalation aromatherapy with lavender essence on pain intensity and anxiety in burn patients: A clinical randomized trial. Avicenna J Nurs Midwifery Care. 2019;26(6):416-27. [View at Publisher] [DOI] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
